

Microbial larvicide application by a large-scale, community-based program reduces malaria infection prevalence in urban Dar es Salaam, Tanzania
- PMID: 19333402
- PMCID: PMC2661378
- DOI: 10.1371/journal.pone.0005107
Microbial larvicide application by a large-scale, community-based program reduces malaria infection prevalence in urban Dar es Salaam, Tanzania
Abstract
Background: Malaria control in Africa is most tractable in urban settlements yet most research has focused on rural settings. Elimination of malaria transmission from urban areas may require larval control strategies that complement adult mosquito control using insecticide-treated nets or houses, particularly where vectors feed outdoors.
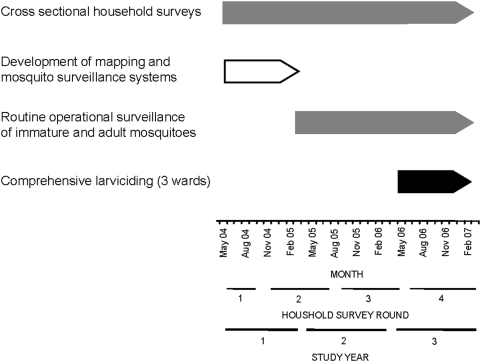
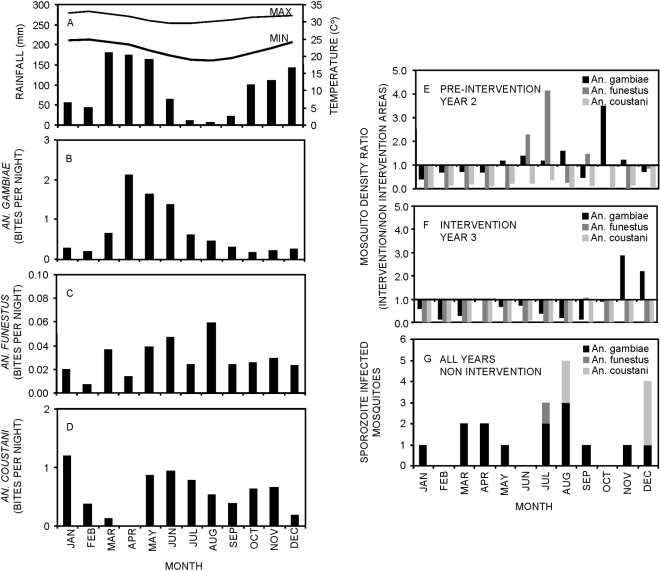
Methods and findings: Microbial larvicide (Bacillus thuringiensis var. israelensis (Bti)) was applied weekly through programmatic, non-randomized community-based, but vertically managed, delivery systems in urban Dar es Salaam, Tanzania. Continuous, randomized cluster sampling of malaria infection prevalence and non-random programmatic surveillance of entomological inoculation rate (EIR) respectively constituted the primary and secondary outcomes surveyed within a population of approximately 612,000 residents in 15 fully urban wards covering 55 km(2). Bti application for one year in 3 of those wards (17 km(2) with 128,000 residents) reduced crude annual transmission estimates (Relative EIR [95% Confidence Interval] = 0.683 [0.491-0.952], P = 0.024) but program effectiveness peaked between July and September (Relative EIR [CI] = 0.354 [0.193 to 0.650], P = 0.001) when 45% (9/20) of directly observed transmission events occurred. Larviciding reduced malaria infection risk among children < or =5 years of age (OR [CI] = 0.284 [0.101 to 0.801], P = 0.017) and provided protection at least as good as personal use of an insecticide treated net (OR [CI] = 0.764 [0.614-0.951], P = 0.016).
Conclusions: In this context, larviciding reduced malaria prevalence and complemented existing protection provided by insecticide-treated nets. Larviciding may represent a useful option for integrated vector management in Africa, particularly in its rapidly growing urban centres.
Conflict of interest statement
Figures




References
-
- Robert V, MacIntyre K, Keating J, Trape JF, Duchemin JB, et al. Malaria transmission in urban sub-Saharan Africa. Am J Trop Med Hyg. 2003;68:169–176. - PubMed
-
- Keiser J, Utzinger J, Castro MC, Smith TA, Tanner M, et al. Urbanization in sub-Saharan Africa and implication for malaria control. Am J Trop Med Hyg. 2004;71:118–127. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
