

Declined neural efficiency in cognitively stable human immunodeficiency virus patients
- PMID: 19334060
- PMCID: PMC2734503
- DOI: 10.1002/ana.21594
Declined neural efficiency in cognitively stable human immunodeficiency virus patients
Abstract
Objective: To determine whether brain activation changes in clinically and neurocognitively normal human immunodeficiency virus (HIV)-infected and in HIV-seronegative control (SN) participants over a 1-year period.
Methods: Functional magnetic resonance imaging (fMRI) was performed in 32 SN and 31 HIV patients (all with stable combination antiretroviral treatment) at baseline and after 1 year. Each participant performed a set of visual attention tasks with increasing attentional load (from tracking two, three, or four balls). All HIV and SN participants had normal neuropsychological function at both examinations.
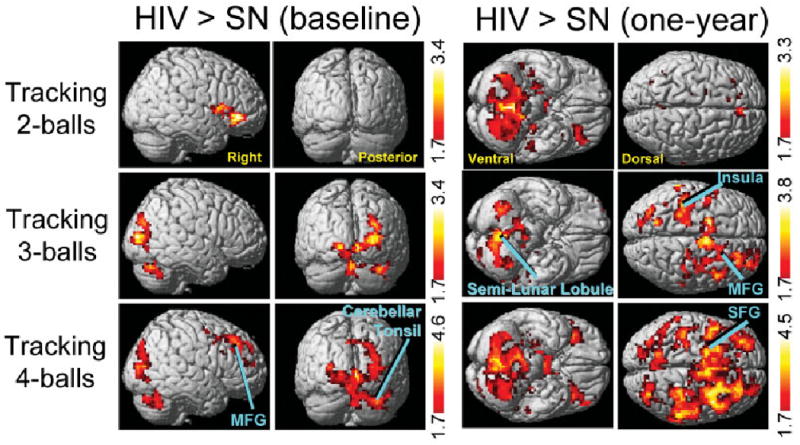
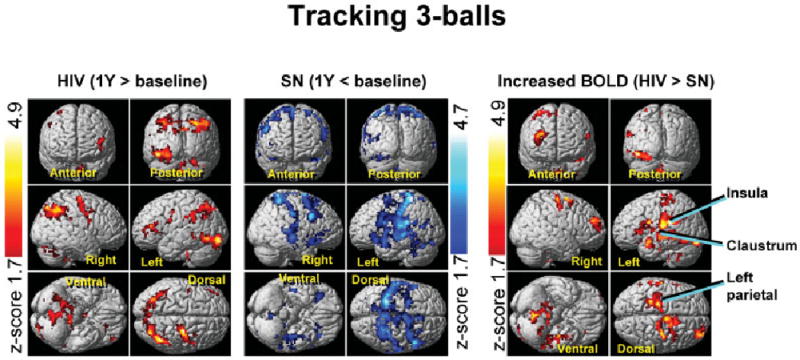
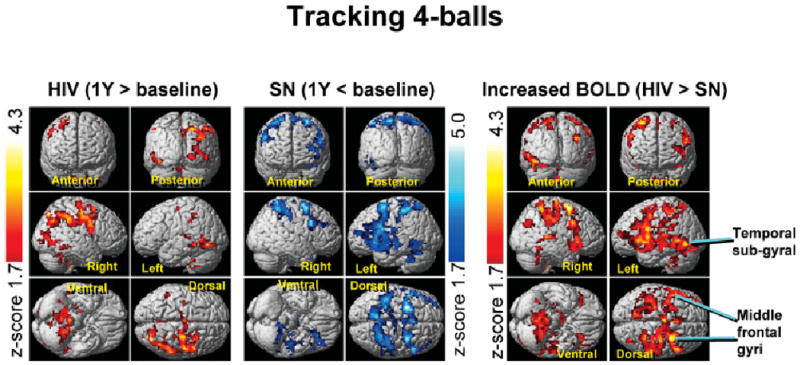
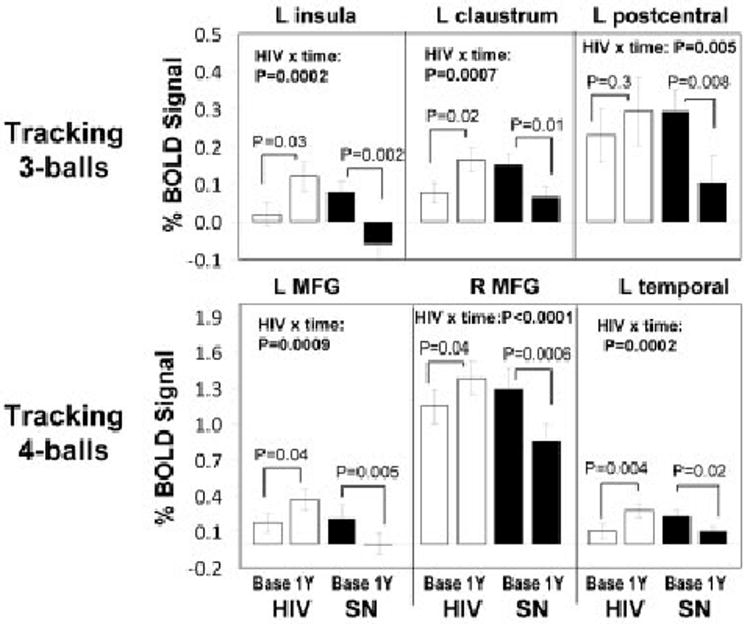
Results: Over 1 year, HIV patients showed no change in their neurocognitive status or in task performance during fMRI. However, HIV patients showed significant 1-year increases in fMRI signals in the prefrontal and posterior parietal cortices for the more difficult tasks, whereas SN control participants showed only decreases in brain activation in these regions. This resulted in significant interactions between HIV status and time of study in left insula, left parietal, left temporal, and several frontal regions (left and right middle frontal gyrus, and anterior cingulate).
Interpretation: Because fMRI task performance remained unchanged in both groups, the HIV patients appeared to maintain performance by increasing usage of the attention network, whereas the control participants reduced usage of the attention network after 1 year. These findings suggest improved efficiency or a practice effect in the SN participants but declined efficiency of the neural substrate in HIV patients, possibly because of ongoing brain injury associated with the HIV infection, despite their apparent stable clinical course.
Conflict of interest statement
Potential conflict of interest: Nothing to report.
Figures
References
-
- Gray F, Adle-Biassette H, Chretien F, et al. Neuropathology and neurodegeneration in human immunodeficiency virus infection Pathogenesis of HIV-induced lesions of the brain, correlations with HIV-associated disorders and modifications according to treatments. Clin Neuropathol. 2001;20:146–155. - PubMed
-
- Janssen RS, Cornblath DR, Epstein LG, et al. Nomenclature and research case definitions for neurologic manifestations of human immunodeficiency virus-type 1 (HIV-1) infection. Neurology. 1991;41:778–785. - PubMed
-
- Dore GJ, McDonald A, Li Y, et al. Marked improvement in survival following AIDS dementia complex in the era of highly active antiretroviral therapy. AIDS. 2003;17:1539–1545. - PubMed
-
- McArthur JC, Haughey N, Gartner S, et al. Human immunodeficiency virus-associated dementia: an evolving disease. J Neurovirol. 2003;9:205–221. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
