

Understanding pharmacist decision making for adverse drug event (ADE) detection
- PMID: 19335483
- PMCID: PMC4401458
- DOI: 10.1111/j.1365-2753.2008.00992.x
Understanding pharmacist decision making for adverse drug event (ADE) detection
Abstract
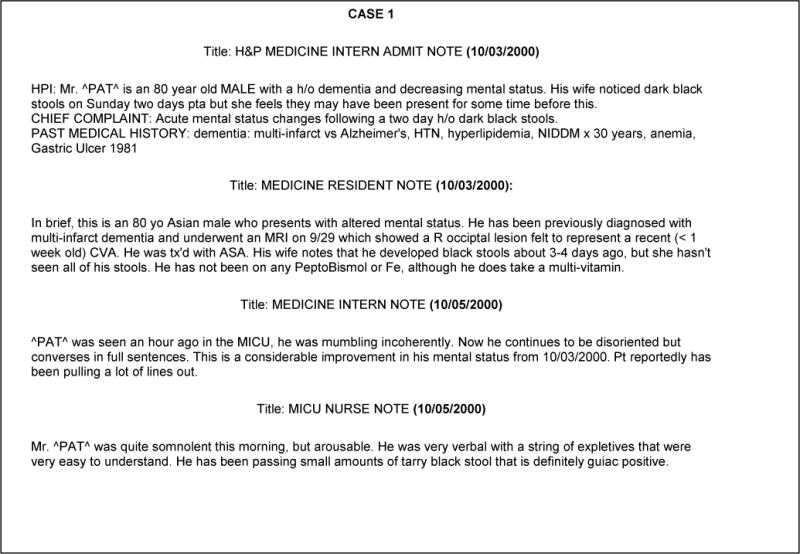
Rationale, aims and objective: Manual chart review is an effective but expensive method for adverse drug event (ADE) detection. Building an expert system capable of mimicking the human expert's decision pathway, to deduce the occurrence of an ADE, can improve efficiency and lower cost. As a first step to build such an expert system, this study explores pharmacist's decision-making processes for ADE detection.
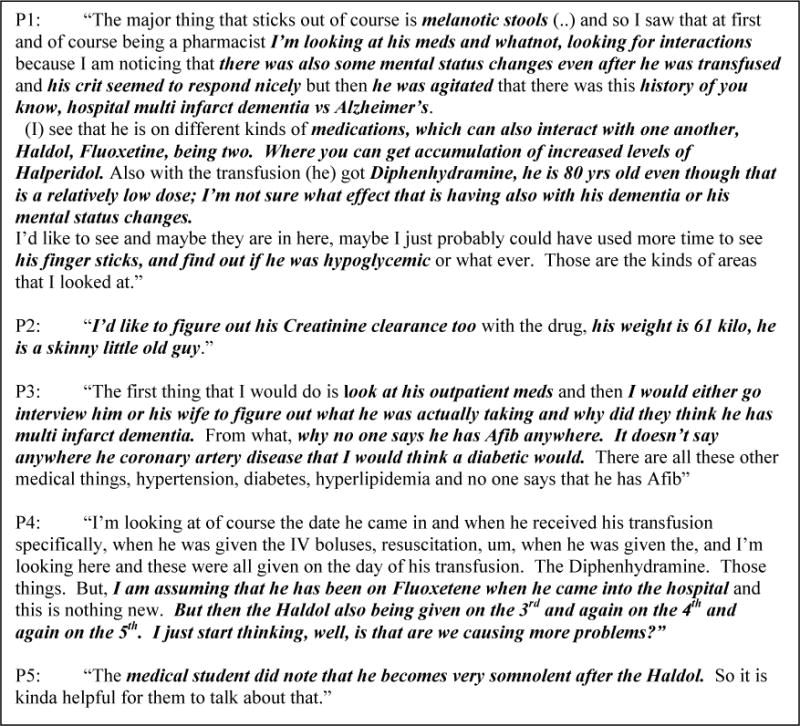
Methods: Think-aloud procedures were used to elicit verbalizations as pharmacists read through ADE case scenarios. Two types of information were extracted, firstly pharmacists' decision-making strategies regarding ADEs and secondly information regarding pharmacists' unmet information needs for ADE detection. Verbal protocols were recorded and analysed qualitatively to extract ADE information signals. Inter-reviewer agreement for classification of ADE information signals was calculated using Cohen's kappa.
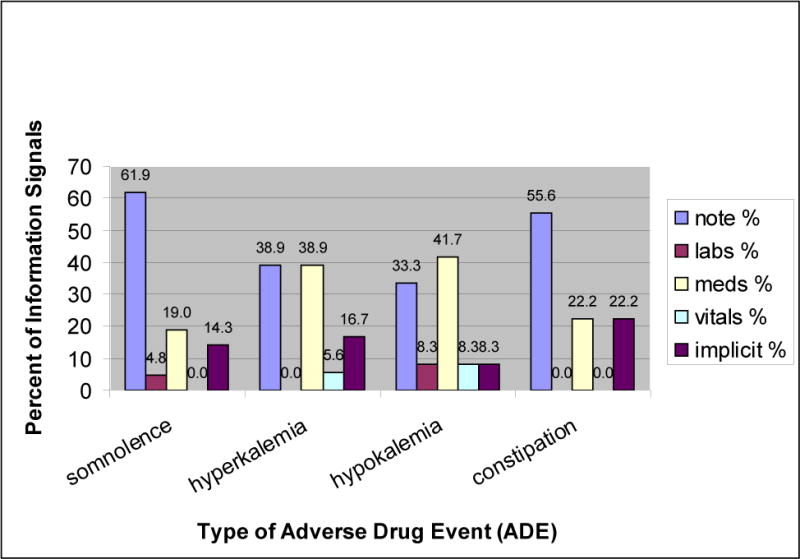
Results: We extracted a total of 110 information signals, of which 73% consisted of information that was interpreted by the pharmacists from the case scenario and only about half (53%, n = 32) of the information signals were considered relevant for the detection of the ADEs. Excellent reliability was demonstrated between the reviewers for classifying signals. Fifty information signals regarding unmet information needs were extracted and grouped into themes based on the type of missing information.
Conclusions: Pharmacists used a forward reasoning approach to make implicit deductions and validate hypotheses about possible ADEs. Verbal protocols also indicated that pharmacists' unmet information needs occurred frequently. Developing alerting systems that meet pharmacists' needs adequately will enhance their ability to reduce preventable ADEs, thus improving patient safety.
Figures
Similar articles
-
Use of verbal protocol analysis for identification of ADE signals.AMIA Annu Symp Proc. 2006;2006:1063. AMIA Annu Symp Proc. 2006. PMID: 17238682 Free PMC article.
-
Hospital admissions caused by adverse drug events: an Australian prospective study.Aust Health Rev. 2014 Feb;38(1):51-7. doi: 10.1071/AH12027. Aust Health Rev. 2014. PMID: 24351707
-
Emergency hospitalizations for adverse drug events in China: Clinical pharmacists' approach to assessment and categorization.Pharmacoepidemiol Drug Saf. 2021 May;30(5):636-643. doi: 10.1002/pds.5215. Epub 2021 Mar 5. Pharmacoepidemiol Drug Saf. 2021. PMID: 33630347
-
Using Electronic Health Records to Identify Adverse Drug Events in Ambulatory Care: A Systematic Review.Appl Clin Inform. 2019 Jan;10(1):123-128. doi: 10.1055/s-0039-1677738. Epub 2019 Feb 20. Appl Clin Inform. 2019. PMID: 30786301 Free PMC article.
-
Pilot testing of checklists to discern adverse drug reactions and adverse drug events.J Am Pharm Assoc (2003). 2013 Jan-Feb;53(1):61-9. doi: 10.1331/JAPhA.2013.11196. J Am Pharm Assoc (2003). 2013. PMID: 23636158 Review.
Cited by
-
A study of deep learning approaches for medication and adverse drug event extraction from clinical text.J Am Med Inform Assoc. 2020 Jan 1;27(1):13-21. doi: 10.1093/jamia/ocz063. J Am Med Inform Assoc. 2020. PMID: 31135882 Free PMC article.
-
Retail pharmacy staff perceptions of design strengths and weaknesses of electronic prescribing.J Am Med Inform Assoc. 2012 Nov-Dec;19(6):1059-65. doi: 10.1136/amiajnl-2011-000779. Epub 2012 Jun 29. J Am Med Inform Assoc. 2012. PMID: 22753809 Free PMC article.
-
Comparison of computerized surveillance and manual chart review for adverse events.J Am Med Inform Assoc. 2011 Jul-Aug;18(4):491-7. doi: 10.1136/amiajnl-2011-000187. J Am Med Inform Assoc. 2011. PMID: 21672911 Free PMC article.
-
Rational and experiential decision-making preferences of third-year student pharmacists.Am J Pharm Educ. 2014 Aug 15;78(6):120. doi: 10.5688/ajpe786120. Am J Pharm Educ. 2014. PMID: 25147392 Free PMC article.
-
Future Directions of Pharmacovigilance Studies Using Electronic Medical Recording and Human Genetic Databases.Toxicol Res. 2019 Oct;35(4):319-330. doi: 10.5487/TR.2019.35.4.319. Epub 2019 Oct 15. Toxicol Res. 2019. PMID: 31636843 Free PMC article. Review.
References
-
- Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. Clinical pharmacists and inpatient medical care: a systematic review. Arch Intern Med. 2006;166(9):955–964. - PubMed
-
- Leape LL, Brennan TA, Laird N, Lawthers AG, Localio AR, Barnes BA, Hebert L, Newhouse JP, Weiler PC, Hiatt H. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med. 1991;324(6):377–384. - PubMed
-
- Nickerson A, MacKinnon NJ, Roberts N, Saulnier L. Drug-therapy problems, inconsistencies and omissions identified during a medication reconciliation and seamless care service. Healthc Q. 2005;8(Spec No):65–72. - PubMed
-
- Gleason KM, Groszek JM, Sullivan C, Rooney D, Barnard C, Noskin GA. Reconciliation of discrepancies in medication histories and admission orders of newly hospitalized patients. Am J Health Syst Pharm. 2004;61(16):1689–1695. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
