

Treatment and prevention of vitamin D insufficiency in cystic fibrosis patients: comparative efficacy of ergocalciferol, cholecalciferol, and UV light
- PMID: 19336509
- PMCID: PMC2690417
- DOI: 10.1210/jc.2008-2012
Treatment and prevention of vitamin D insufficiency in cystic fibrosis patients: comparative efficacy of ergocalciferol, cholecalciferol, and UV light
Abstract
Background: The optimal treatment for correcting or preventing vitamin D insufficiency in cystic fibrosis (CF) patients has not been established.
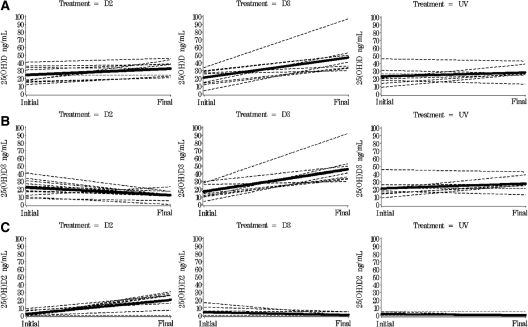
Objective: The aim of the study was to assess the relative efficacy of three modes of vitamin D therapy: cholecalciferol (D3), ergocalciferol (D2), and UV light in raising or maintaining 25(OH)D levels above 30 ng/ml.
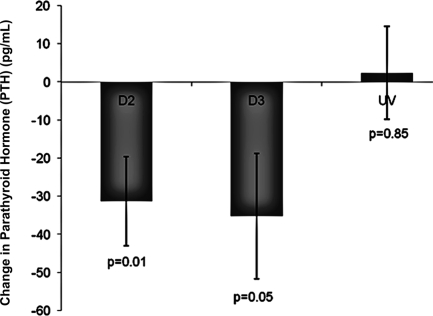
Design: Thirty adult CF subjects with vitamin D insufficiency were randomized into one of three treatment arms: D3, D2, or UV light. Subjects randomized to D3 or D2 ingested 50,000 IU of vitamin D weekly, and those randomized to UV exposed their skin to UV light from a lamp five times a week. Serum was collected for 25(OH)D and PTH at baseline and at 12 wk.
Results: Treatment with D3 and D2 raised 25(OH)D levels significantly, from a mean of 21.2 +/- 10.18 to 47.1 +/- 20.5 ng/ml (P < 0.001) and 24.4 +/- 10.3 to 32.7+/- 9.7 ng/ml (P = 0.01), with 100% and 60% reaching 25(OH)D levels above 30 ng/ml, respectively. Treatment with UV did not raise 25(OH)D levels significantly; however, only 55% of subjects were adherent with UV therapy.
Conclusion: This study demonstrates that CF subjects are able to achieve or maintain optimal vitamin D status (>30 ng/ml) with two oral regimens of either D3 or D2 treatment, the former being more efficacious. A confounding variable for this observation is the fact that the D3 and D2 capsules contained different carriers, powder-based vs. oil-based, respectively. UV therapy did not alter vitamin D status, possibly due to poor adherence to UV therapy.
Figures
References
-
- Rovner AJ, Stallings VA, Schall JI, Leonard MB, Zemel BS 2007 Vitamin D insufficiency in children, adolescents, and young adults with cystic fibrosis despite routine oral supplementation. Am J Clin Nutr 86:1694–1699 - PubMed
-
- Looker AC, Dawson-Hughes B, Calvo MS, Gunter EW, Sahyoun NR 2002 Serum 25-hydroxyvitamin D status of adolescents and adults in two seasonal subpopulations from NHANES III. Bone 30:771–777 - PubMed
-
- Stephenson A, Brotherwood M, Robert R, Atenafu E, Corey M, Tullis E 2007 Cholecalciferol significantly increases 25-hydroxyvitamin D concentrations in adults with cystic fibrosis. Am J Clin Nutr 85:1307–1311 - PubMed
