

Neurosurgical strategies for Gilles de la Tourette's syndrome
- PMID: 19337454
- PMCID: PMC2646643
- DOI: 10.2147/ndt.s4160
Neurosurgical strategies for Gilles de la Tourette's syndrome
Abstract
Tourette's syndrome (TS) is a neurological disorder characterized by motor and vocal tics that typically begin in childhood and often are accompanied by psychiatric comorbidities. Symptoms of TS may be socially disabling and cause secondary medical complications. Pharmacological therapies remain the mainstay of symptom management. For the subset of patients in whom TS symptoms are medically recalcitrant and do not dissipate by adulthood, neurosurgery may offer an alternative treatment strategy. Greater understanding of the neuroanatomic and pathophysiologic basis of TS has facilitated the development of surgical procedures that aim to ameliorate TS symptoms by lesions or deep brain stimulation of cerebral structures. Herein, the rationale for the surgical management of TS is discussed and neurosurgical experiences since the 1960s are reviewed. The necessity for neurosurgical strategies to be performed with appropriate ethical considerations is highlighted.
Keywords: deep brain stimulation; neurosurgery; thalamus; tourette’s syndrome.
Figures
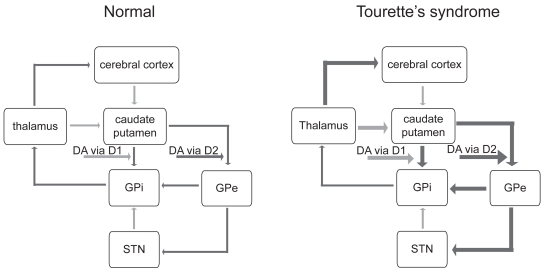
 and inhibitory (GAB-Aergic) projections →. Normally, dopamine, acting via D1 dopamine receptors, has an excitatory influence on striatal projections to the GPi and, acting via D2 dopamine receptors, an inhibitory influence on striatal projections to the GPe, maintaining a balance between the activities of the direct and indirect basal ganglia pathways. According to the dopaminergic hypothesis of TS pathophysiology, dopaminergic hyperactivity causes increased activity in the direct pathway (indicated by the heavier weighted lines) and decreased activity in the indirect pathway, which serves to enhance thalamocortical activity. In TS, the thalamus, caudate-putamen, and GPe become pathologically hyperactive, and the GPi and STN become pathologically hypoactive. Abbreviations: GPi, globus pallidus pars internus; GPe, globus pallidus pars externus; STN, subthalamic nucleus; DA, dopamine.
and inhibitory (GAB-Aergic) projections →. Normally, dopamine, acting via D1 dopamine receptors, has an excitatory influence on striatal projections to the GPi and, acting via D2 dopamine receptors, an inhibitory influence on striatal projections to the GPe, maintaining a balance between the activities of the direct and indirect basal ganglia pathways. According to the dopaminergic hypothesis of TS pathophysiology, dopaminergic hyperactivity causes increased activity in the direct pathway (indicated by the heavier weighted lines) and decreased activity in the indirect pathway, which serves to enhance thalamocortical activity. In TS, the thalamus, caudate-putamen, and GPe become pathologically hyperactive, and the GPi and STN become pathologically hypoactive. Abbreviations: GPi, globus pallidus pars internus; GPe, globus pallidus pars externus; STN, subthalamic nucleus; DA, dopamine.
Similar articles
-
[Control of inner speech and Gilles de la Tourette's syndrome].Encephale. 2003 Sep-Oct;29(5):460-2. Encephale. 2003. PMID: 14615696 French.
-
The use of deep brain stimulation in Tourette's syndrome.Neurosurg Focus. 2013 Nov;35(5):E4. doi: 10.3171/2013.8.FOCUS13292. Neurosurg Focus. 2013. PMID: 24175864 Review.
-
Deep brain stimulation in Tourette's syndrome: evidence to date.Neuropsychiatr Dis Treat. 2019 Apr 29;15:1061-1075. doi: 10.2147/NDT.S139368. eCollection 2019. Neuropsychiatr Dis Treat. 2019. PMID: 31114210 Free PMC article. Review.
-
Efficacy of Behavioural Intervention, Antipsychotics, and Alpha Agonists in the Treatment of Tics Disorder in Tourette's Syndrome.Cureus. 2022 Feb 21;14(2):e22449. doi: 10.7759/cureus.22449. eCollection 2022 Feb. Cureus. 2022. PMID: 35345730 Free PMC article. Review.
-
Costs of control: decreased motor cortex engagement during a Go/NoGo task in Tourette's syndrome.Brain. 2014 Jan;137(Pt 1):122-36. doi: 10.1093/brain/awt288. Epub 2013 Oct 30. Brain. 2014. PMID: 24176975
References
-
- Ackermans L, Temel Y, Bauer NJC, et al. Vertical gaze palsy after thalamic stimulation for Tourette syndrome: case report. Neurosurgery. 2007;61:E1100. - PubMed
-
- Ackermans L, Temel Y, Cath D, et al. Deep brain stimulation for Tourette’s syndrome: two targets? Mov Disord. 2006;21:709–13. - PubMed
-
- Albin RL, Koeppe RA, Bohnen NI, et al. Increased ventral striatal monoaminergic innervations in Tourette syndrome. Neurology. 2003;61:310–5. - PubMed
-
- Alex KD, Yavanian GJ, McFarlane HG, et al. Modulation of dopamine release by striatal 5-HT2C receptors. Synapse. 2005;55:242–51. - PubMed
-
- Alexander GE, DeLong MR. Microstimulation of the primate striatum. II. Somatotopic organization of striatal microexcitable zones and their relation to neuronal response properties. J Neurophysiol. 1985;53:1417–30. - PubMed
LinkOut - more resources
Full Text Sources
