

Update on the use of trandolapril in the management of cardiovascular disorders
- PMID: 19337528
- PMCID: PMC2663436
- DOI: 10.2147/vhrm.s3467
Update on the use of trandolapril in the management of cardiovascular disorders
Abstract
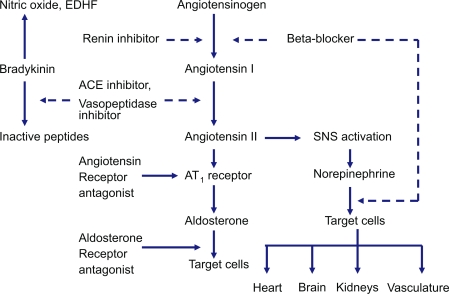
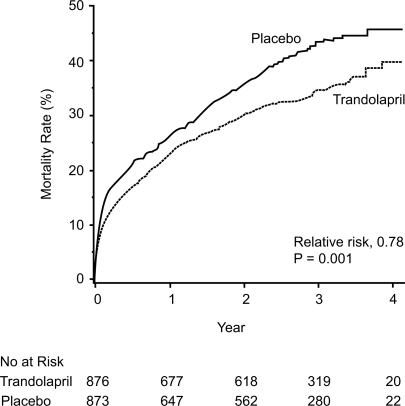
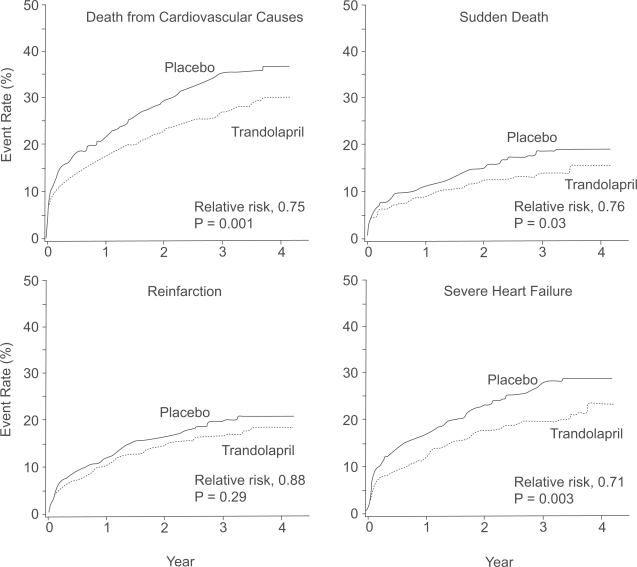
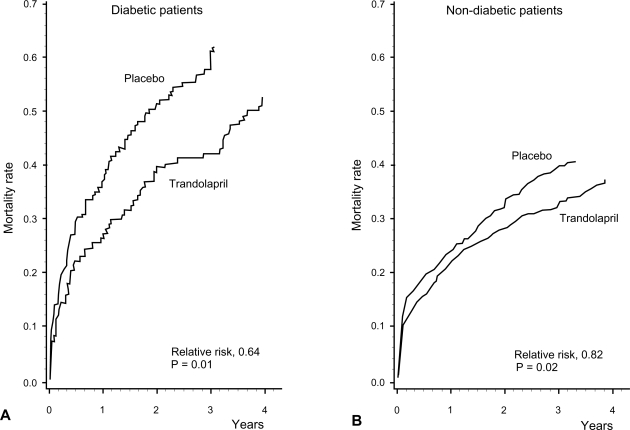
Trandolapril is a well known angiotensin converting enzyme (ACE) inhibitor with many cardiovascular (CV) indications. The objectives of this article are to review the pharmacokinetics and pharmacodynamics properties of trandolapril and to focus on its clinical relevance in cardiovascular medicine. Various populations have been studied in large clinical trials including patients with congestive heart failure (CHF) after an acute myocardial infarction (AMI), diabetics, patients with hypertension (HTN), stable coronary artery disease (CAD) and prevention of proteinuria. Long-term treatment with trandolapril in patients with reduced left ventricular function soon after AMI significantly reduced the risk of overall mortality, mortality from CV causes, sudden death, and the development of severe CHF. Treatment with trandolapril after AMI complicated by left ventricular dysfunction appears to be of considerable importance in patients with diabetes mellitus by saving lives and substantially reducing the risk of progression to severe CHF as well. Moreover, trandolapril reduces progression to proteinuria in high-risk patients. Some of the advantages of trandolapril over other ACE inhibitors are the wide spectrum of patient populations studied, the well established dosage and its proven trough-to-peak effect ratios permitting a safe once-a-day administration.
Keywords: angiotensin converting enzyme inhibitors; diabetic nephropathy; hypertension cardiovascular diseases; trandolapril.
Figures

References
-
- Agewall S, Wikstrand J, Ljungman S, et al. Usefulness of microalbuminuria in predicting cardiovascular mortality in treated hypertensive men with and without diabetes mellitus. Risk Factor Intervention Study Group. Am J Cardiol. 1997;80:164–9. - PubMed
-
- Amann K, Irzyniec T, Mall G, et al. The effect of enalapril on glomerular growth and glomerular lesions after subtotal nephrectomy in the rat: a stereological analysis. J Hypertens. 1993;11:969–75. - PubMed
-
- Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:e1–e157. - PubMed
-
- Arner P, Wade A, Engfeldt P, et al. Pharmacokinetics and pharmacodynamics of trandolapril after repeated administration of 2 mg to young and elderly patients with mild-to-moderate hypertension. J Cardiovasc Pharmacol. 1994;23(Suppl 4):S44–9. - PubMed
-
- Aurell M. The renin-angiotensin system: the centenary jubilee. Blood Press. 1998;7:71–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
