

The evolution of systolic blood pressure as a strong predictor of cardiovascular risk and the effectiveness of fixed-dose ARB/CCB combinations in lowering levels of this preferential target
- PMID: 19337545
- PMCID: PMC2663439
- DOI: 10.2147/vhrm.s4073
The evolution of systolic blood pressure as a strong predictor of cardiovascular risk and the effectiveness of fixed-dose ARB/CCB combinations in lowering levels of this preferential target
Abstract
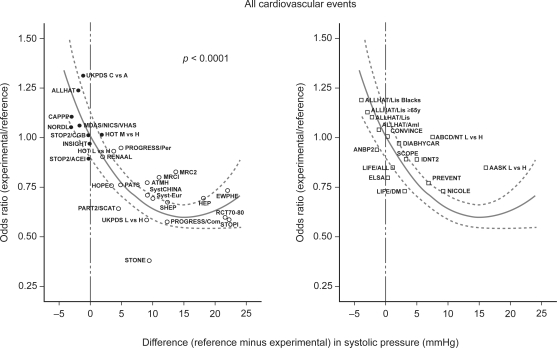
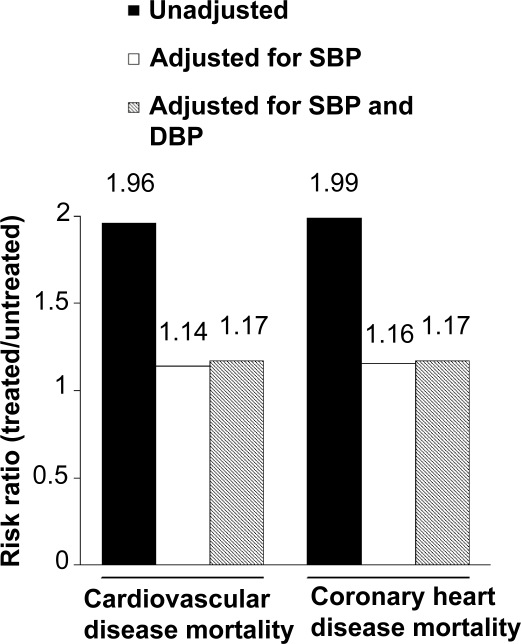
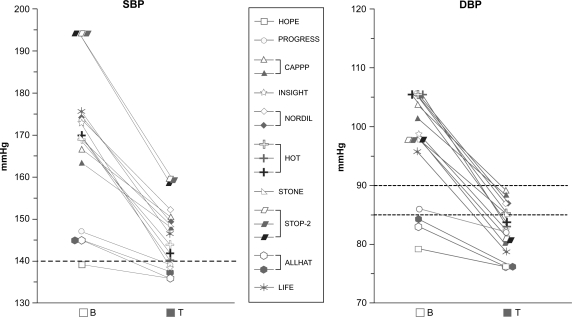
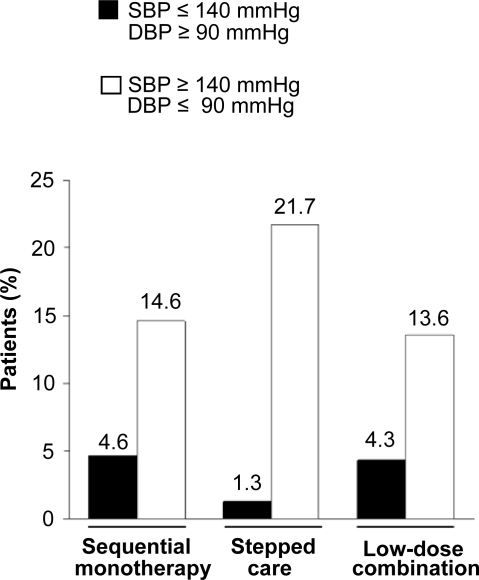
Elevated blood pressure is an important cardiovascular risk factor. Although targets for both diastolic blood pressure (DBP) and systolic blood pressure (SBP) are defined by current guidelines, DBP has historically taken precedence in hypertension management. However, there is strong evidence that SBP is superior to DBP as a predictor of cardiovascular events. Moreover, achieving control of SBP is assuming greater importance amongst an aging population. In spite of the growing recognition of the importance of SBP in reducing cardiovascular risk and the emphasis by current guidelines on SBP control, a substantial proportion of patients still fail to achieve SBP targets, and SBP control is achieved much less frequently than DBP control. Thus, new approaches to the management of hypertension are required in order to control SBP and minimize cardiovascular risk. Fixed-dose combination (FDC) therapy is an approach that offers the advantages of multiple drug administration and a reduction in regimen complexity that favors compliance. We have reviewed the latest evidence demonstrating the efficacy in targeting SBP of the most recent FDC products; combinations of the calcium channel blocker (CCB), amlodipine, with angiotensin receptor blockers (ARBs), valsartan or olmesartan. In addition, results from studies with new classes of agent are outlined.
Keywords: angiotensin receptor blocker; calcium channel blocker; combination therapy; hypertension; systolic blood pressure.
Figures
References
-
- Bangalore S, Kamalakkannan G, Parkar S, et al. Fixed-dose combinations improve medication compliance: a meta-analysis. Am J Med. 2007;120:713–9. - PubMed
-
- Benetos A, Thomas F, Bean KE, et al. Why cardiovascular mortality is higher in treated hypertensives versus subjects of the same age, in the general population. J Hypertens. 2003;21:1635–40. - PubMed
-
- Benetos A, Thomas F, Safar ME, et al. Should diastolic and systolic blood pressure be considered for cardiovascular risk evaluation: a study in middle-aged men and women. J Am Coll Cardiol. 2000;37:163–8. - PubMed
-
- Black HR, Elliott WJ, Neaton JD, et al. Baseline characteristics and early blood pressure control in the CONVINCE Trial. Hypertension. 2001;37:12–18. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
