

Anabolic steroids, acute myocardial infarction and polycythemia: a case report and review of the literature
- PMID: 19337562
- PMCID: PMC2663437
- DOI: 10.2147/vhrm.s4261
Anabolic steroids, acute myocardial infarction and polycythemia: a case report and review of the literature
Abstract
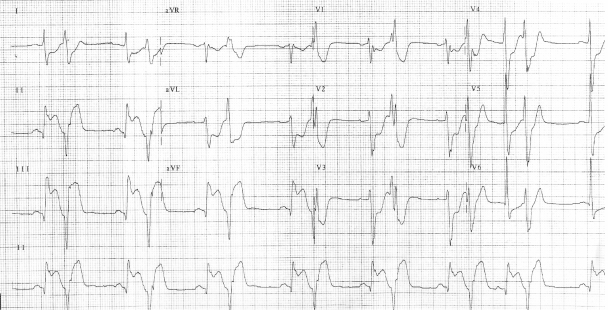
The association between testosterone-replacement therapy and cardiovascular risk remains unclear with most reports suggesting a neutral or possibly beneficial effect of the hormone in men and women. However, several cardiovascular complications including hypertension, cardiomyopathy, stroke, pulmonary embolism, fatal and nonfatal arrhythmias, and myocardial infarction have been reported with supraphysiologic doses of anabolic steroids. We report a case of an acute ST-segment elevation myocardial infarction in a patient with traditional cardiac risk factors using supraphysiologic doses of supplemental, intramuscular testosterone. In addition, this patient also had polycythemia, likely secondary to high-dose testosterone. The patient underwent successful percutaneous intervention of the right coronary artery. Phlebotomy was used to treat the polycythemia acutely. We suggest that the chronic and recent "stacked" use of intramuscular testosterone as well as the resultant polycythemia and likely increased plasma viscosity may have been contributing factors to this cardiovascular event, in addition to traditional coronary risk factors. Physicians and patients should be aware of the clinical consequences of anabolic steroid abuse.
Keywords: acute myocardial infarction; anabolic steroid use; polycythemia.
Figures



References
-
- Ajayi AAL, Mathur R, Halushka PV. Testosterone increase human platelet thromboxane A2 receptor density and aggregation responses. Circulation. 1995;91:2742–7. - PubMed
-
- Basaria S, Dobs AS. Risks versus benefits of testosterone therapy in elderly men. Drugs Aging. 1999;15:131–42. - PubMed
-
- Choi BG, McLaughlin MA. Why men’s hearts break: cardiovascular effects of sex steroids. Endocrinol Metab Clin N Am. 2007;36:365–77. - PubMed
-
- Dhar R, Stout W, Link MS, et al. Cardiovascular toxicities of performance-enhancing substances in sports. Mayo Clin Proc. 2005;80:1307–15. - PubMed
-
- Dobs AS, Meikle AW, Arver S, et al. Pharmacokinetics, efficacy, and safety of a permeation-enhanced testerosterone in comparison with bi-weekly injections of testerosterone enanthate for the treatment of hypogonadal men. J Clin Endocrinol Metab. 1999;64:3469–78. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
