

Cementless total hip replacement: past, present, and future
- PMID: 19337818
- PMCID: PMC2779384
- DOI: 10.1007/s00776-008-1317-4
Cementless total hip replacement: past, present, and future
Abstract
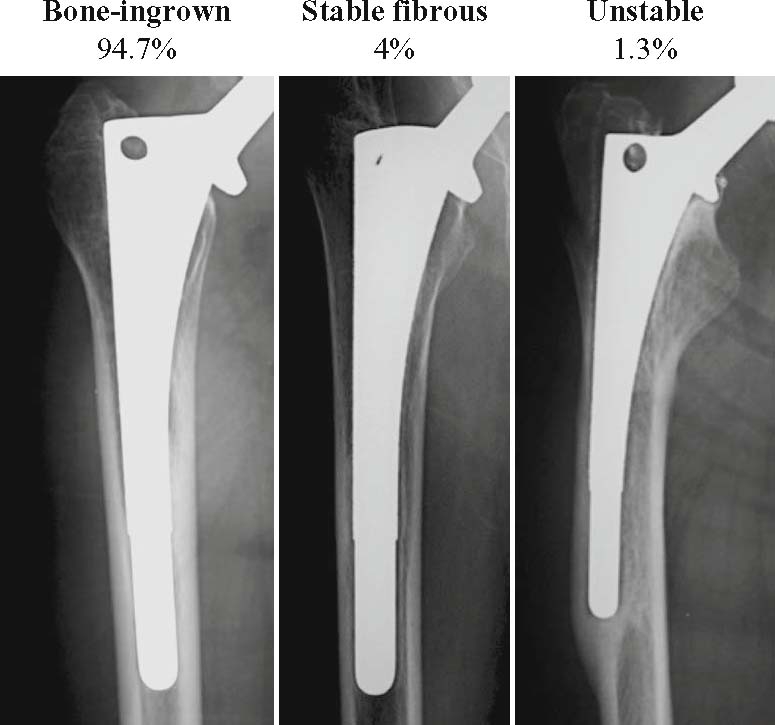
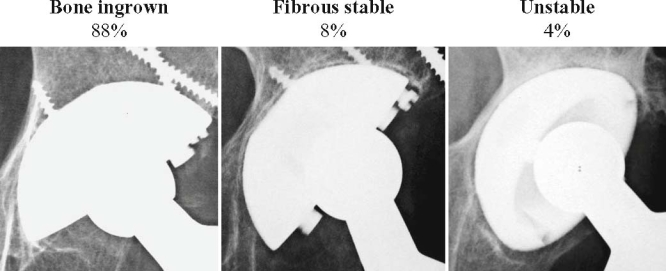
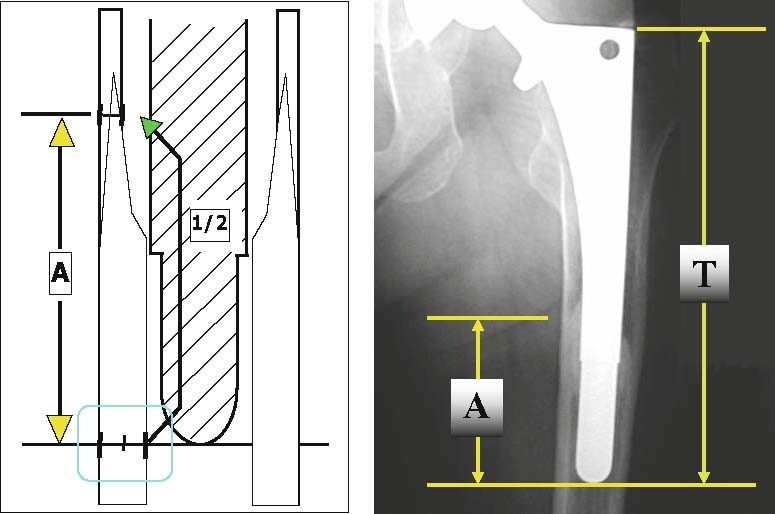
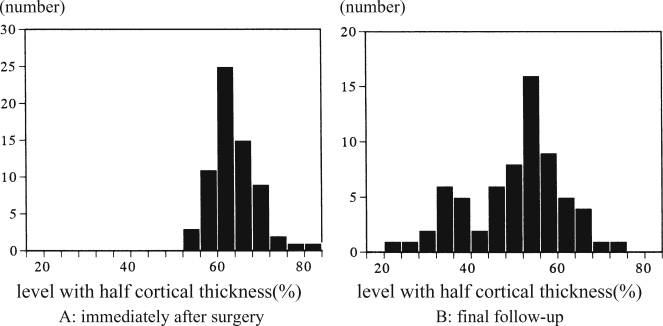
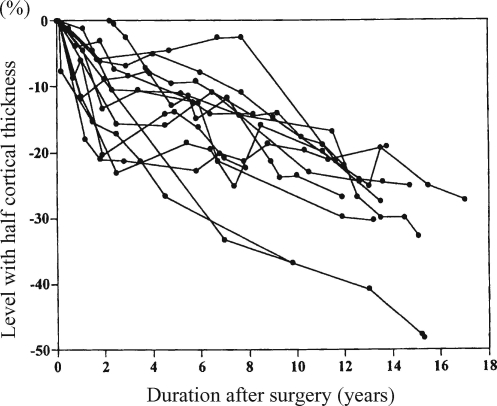
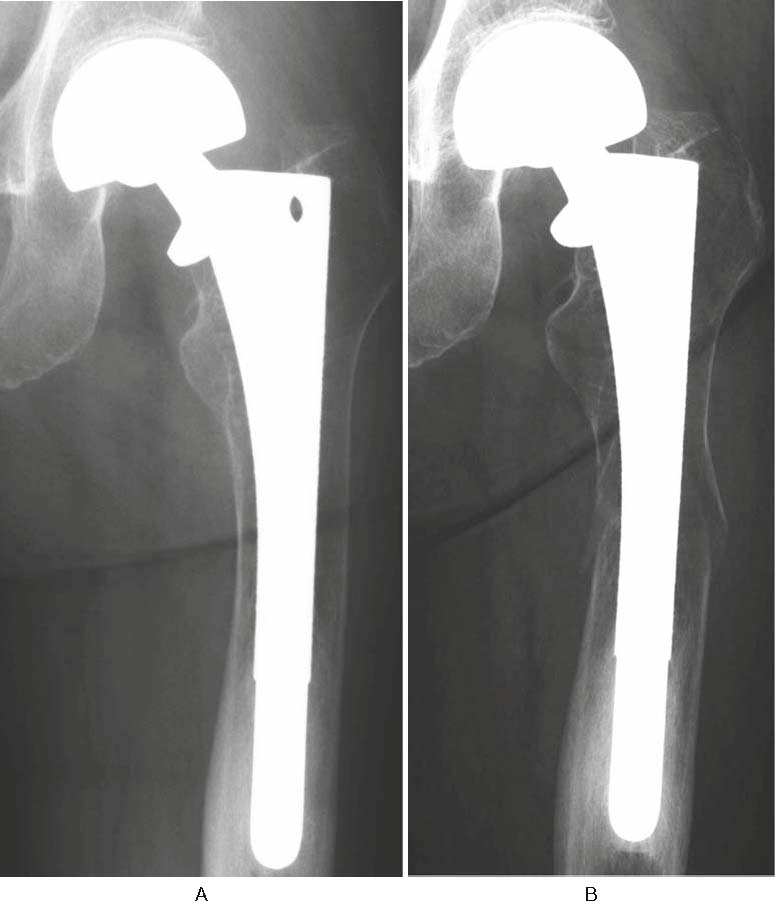
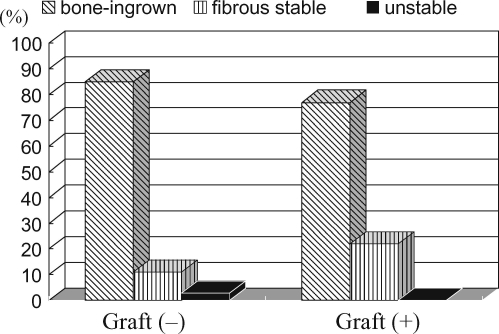
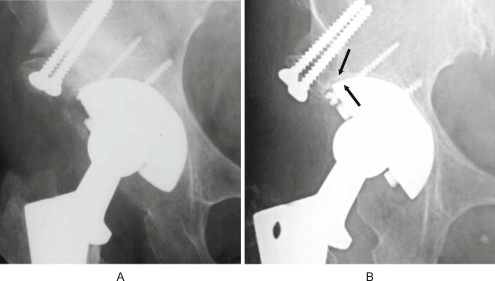
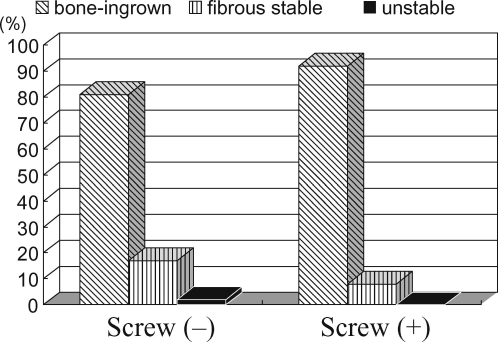
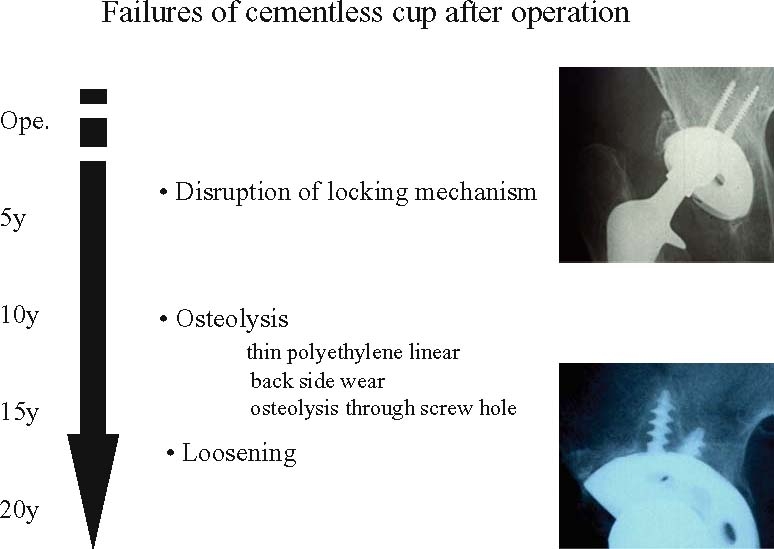
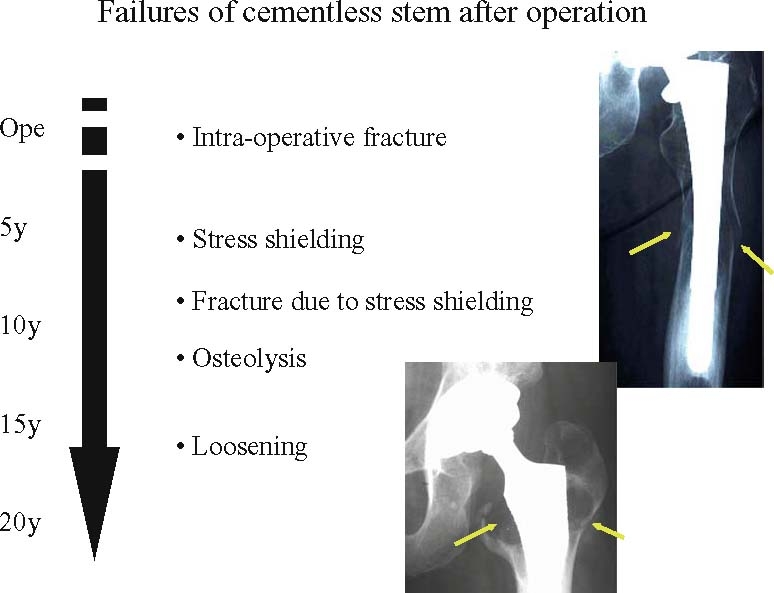
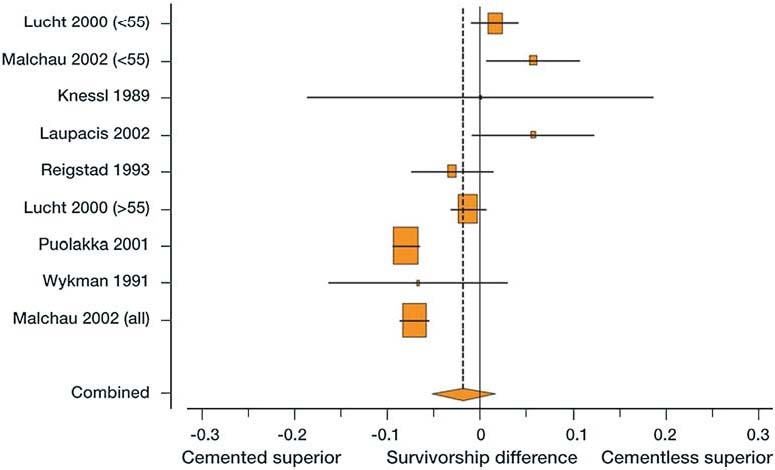
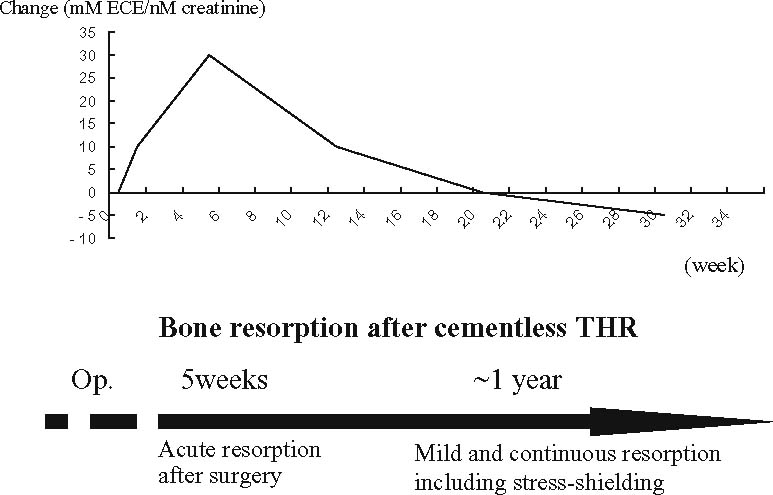
Cementless total hip replacement (THR) is rapidly being accepted as the surgery for arthritic diseases of the hip joint. The bone-ingrowth rate in porous-type cementless implants was about 90% over 10 years after surgery, showing that biological fixation of cementless THR was well maintained on both the stem and cup sides. As for the stress shielding of the femur operated using a distal fixation-type stem, severe bone resorption was observed. The severe bone resorption group showed continuous progression for more than 10 years after surgery. Stem loosening directly caused by stress shielding has been considered less likely; however, close attention should be paid to bone resorption-associated disorders including femoral fracture. Cementless cups have several specific problems. It is difficult to decide whether a cup should be placed in the physiological position for the case of acetabular dysplasia by bone grafting or at a relatively higher position without bone grafting. The bone-ingrowth rate was lower in the group with en bloc bone grafting, and the reactive line was frequently noted in the bone-grafted region. Although no data indicated that en bloc bone grafting directly led to poor outcomes, such as loosening, cup placement at a higher site without bone grafting is now selected by most operators. The polyethylene liner in a cementless cup is thinned due to the metal cup thickness; however, it has been suggested that the apparent relation between the cup size and the wear rate was absent as long as a cementless cup is used. Comparative study indicated cementless THR was inferior with regard to the yearly polyethylene wear rate and incidence of osteolysis on both the stem and cup sides. Meta-analysis study on the survival rate between cement and cementless THR reported that cemented THR was slightly superior. It should be considered that specific problems for cementless THR, especially with regard to polyethylene wear, do occur.
Figures

References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00003086-200112000-00016', 'is_inner': False, 'url': 'https://doi.org/10.1097/00003086-200112000-00016'}, {'type': 'PubMed', 'value': '11764343', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11764343/'}]}
- Engh CA Jr, Claus AM, Hopper RH Jr, Engh CA. Long-term results using the anatomic medullary locking hip prosthesis. Clin Orthop 2001;393:137–146. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '12068417', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/12068417/'}]}
- Engh CA, Hopper RH Jr. The odyssey of porous-coated fixation. J Arthroplasty 2002;17(suppl 1):102–107. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '14960669', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/14960669/'}]}
- Gaffey JL, Callaghan JJ, Pedersen DR, Goetz DD, Sullivan PM, Johnston RC. Cementless acetabular fixation at fifteen years: a comparison with the same surgeon’s results following acetabular fixation with cement. J Bone Joint Surg Am 2004;86:257–261. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '5937593', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/5937593/'}]}
- McKee GK, Watson-Farrar J. Replacement of arthritic hips by the McKee-Farrar prosthesis. J Bone Joint Surg Br 1966;48:245–259. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/S0140-6736(61)92063-3', 'is_inner': False, 'url': 'https://doi.org/10.1016/s0140-6736(61)92063-3'}, {'type': 'PubMed', 'value': '15898154', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15898154/'}]}
- Charnley J. Arthroplasty of the hip: a new operation. Lancet 1961;1:1129–1132. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
