

Dose-finding study of 153Sm-EDTMP in patients with poor-prognosis osteosarcoma
- PMID: 19338063
- PMCID: PMC2974628
- DOI: 10.1002/cncr.24286
Dose-finding study of 153Sm-EDTMP in patients with poor-prognosis osteosarcoma
Abstract
Background: Samarium-153 ethylenediaminetetramethylene phosphonic acid ((153)Sm-EDTMP) has been used to treat patients with high-risk osteosarcoma. The purpose of the current study was to determine the maximally tolerated dose of (153)Sm-EDTMP that permits hematopoietic recovery within 6 weeks.
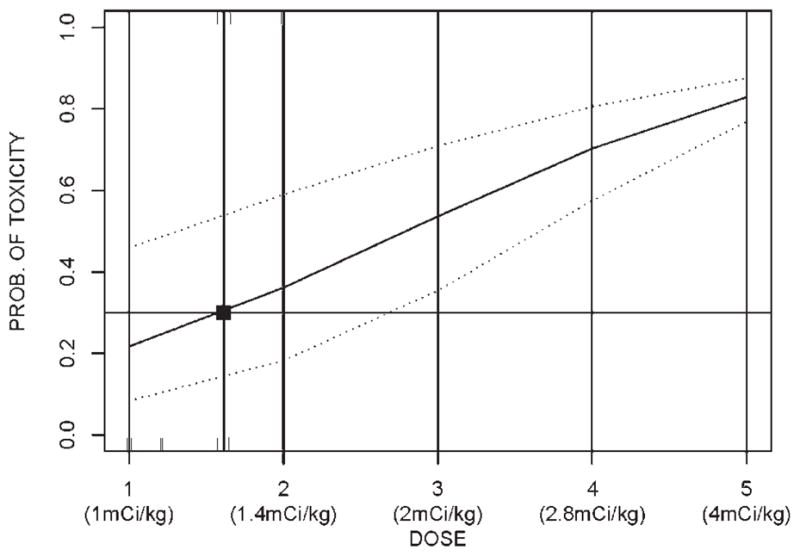
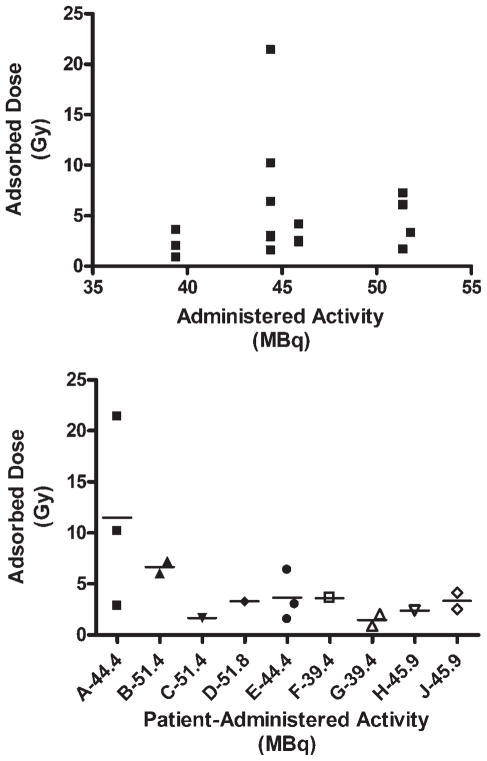
Methods: Patients with recurrent or refractory osteosarcoma with bone metastases were enrolled in this study. Subjects were treated with increasing doses of (153)Sm-EDTMP, beginning with 1.0 millicuries (mCi)/kg and followed initially with 40% increment dose level escalations, using a continual reassessment method for dose escalation and de-escalation with a target dose-limiting toxicity (DLT) rate of 30%. Complete blood counts were monitored weekly, and the primary DLT was defined as failure to achieve an absolute neutrophil count >750/mm(3) and a platelet count >75,000/mm(3) within 6 weeks of treatment. In addition to assessing toxicity, dosimetry measurements were made to estimate the radiation dose delivered to target lesions.
Results: The maximally tolerated dose of (153)Sm-EDTMP was 44.8 megabecquerel (MBq)/kg (1.21 mCi/kg). DLTs were confined to hematologic toxicities, particularly delayed platelet recovery in 2 patients treated at a dose of 51.8 MBq/kg (1.4 mCi/kg). Grade 2 and 3 pulmonary toxicity (graded according to the National Cancer Institute Common Toxicity Criteria [version 3.0]) as reported in 2 patients (at administered activities of 44.8 MBq/kg and 51.8 MBq/kg) was attributable to progressive pulmonary disease. No other significant nonhematologic toxicities were observed.
Conclusions: Patients with osteosarcoma who have previously been heavily treated with chemotherapy can be safely administered (153)Sm-EDTMP with rapid hematologic recovery. The data from the current study support the development of a future trial to assess the efficacy of combining targeted radiotherapy with cytotoxic chemotherapy as a treatment option for patients with high-risk osteosarcoma.
(c) 2009 American Cancer Society.
Conflict of interest statement
Financial support for this study was provided by EUSA Pharma (USA) Inc (Formerly Cytogen Corp.).
Figures
References
-
- Link MP, Goorin AM, Miser AW, et al. The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med. 1986;314:1600–1606. - PubMed
-
- Francis KC, Phillips R, Nickson JJ, Woodard HQ, Higin-botham NL, Coley BL. Massive preoperative irradiation in the treatment of osteogenic sarcoma in children; a preliminary report. Am J Roentgenol Radium Ther Nucl Med. 1954;72:813–818. - PubMed
-
- Jenkin RD, Allt WE, Fitzpatrick PJ. Osteosarcoma. An assessment of management with particular reference to primary irradiation and selective delayed amputation. Cancer. 1972;30:393–400. - PubMed
-
- Lee ES, Mackenzie DH. Osteosarcoma. A study of the value of preoperative megavoltage radiotherapy. Br J Surg. 1964;51:252–274. - PubMed
-
- Machak GN, Tkachev SI, Solovyev YN, et al. Neoadjuvant chemotherapy and local radiotherapy for high-grade osteosarcoma of the extremities. Mayo Clin Proc. 2003;78:147–155. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
