

Prospective assessment of systemic therapy followed by surgical removal of metastases in selected patients with renal cell carcinoma
- PMID: 19338544
- PMCID: PMC4464661
- DOI: 10.1111/j.1464-410X.2009.08490.x
Prospective assessment of systemic therapy followed by surgical removal of metastases in selected patients with renal cell carcinoma
Abstract
Objective: To prospectively establish objective selection criteria for metastasectomy in patients with metastatic renal cell carcinoma (mRCC).
Patients and methods: Between 1991 and 1999, 38 patients with mRCC with responsive or stable disease after initial systemic therapy, and with potentially resectable disease, were enrolled. Patients had a metastasectomy with curative intent and received consolidative adjuvant systemic therapy.
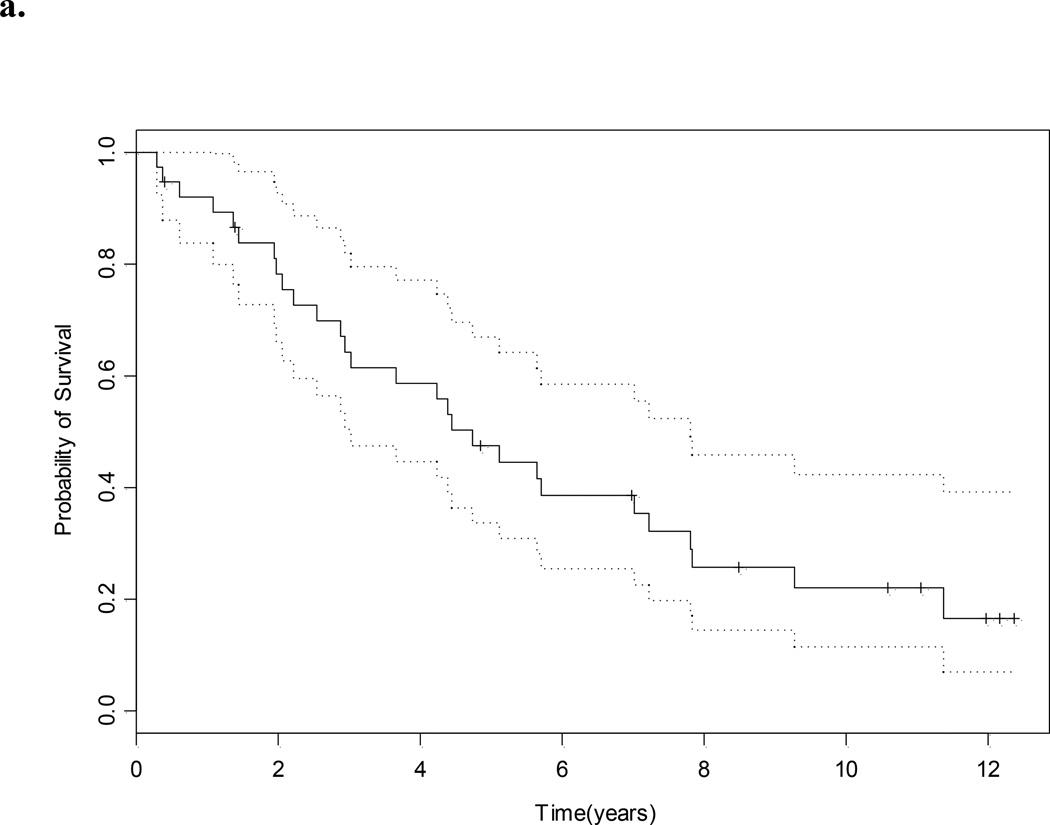
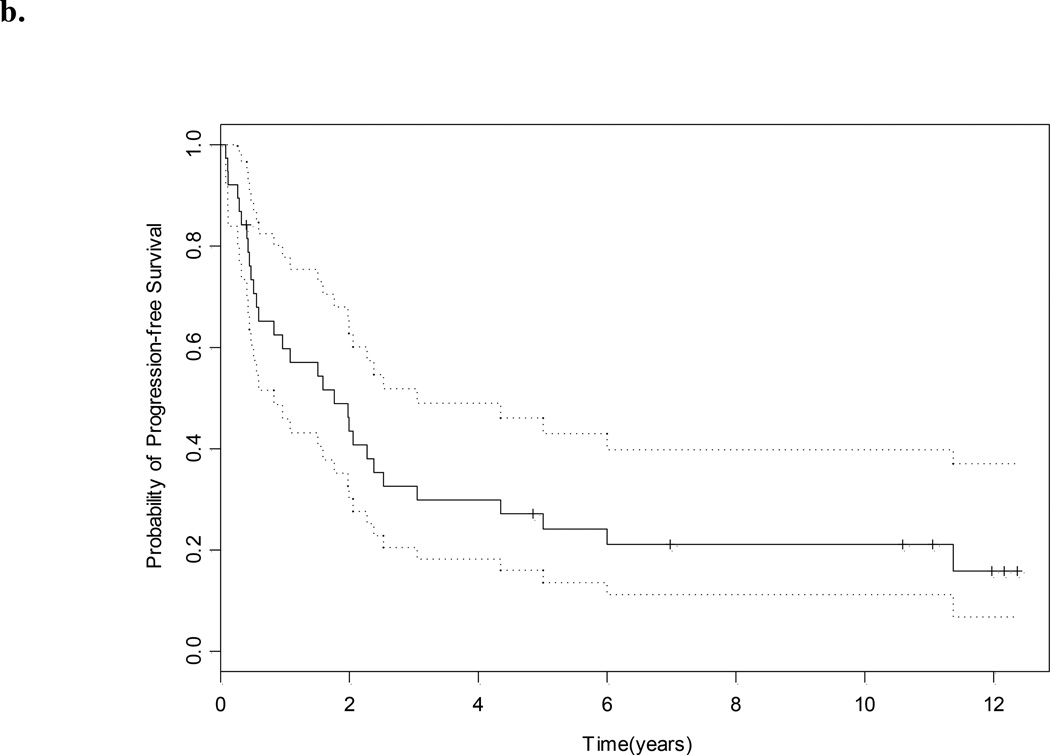
Results: Of the patients enrolled, 79% had stable disease after initial systemic therapy and 21% had a partial or complete response. Most (84%) had metastasectomy of one organ site. There was surgically no evidence of disease (sNED) in 76%. Operative morbidity and mortality were acceptable and 90% of the patients received adjuvant systemic therapy. The median (95% confidence interval) survival was 4.7 (3.0-7.8) years, and the median time to progression was 1.8 (0.8-3.1) years. Eight of 38 patients (21%) remained free of disease by the end of the study. Significant predictors of outcome were lack of sNED after metastasectomy, and the presence of pulmonary metastases. The median overall survival for those who had sNED was 5.6 years, vs 1.4 years for those who did not (P < 0.001).
Conclusions: Metastasectomy in patients with mRCC not progressing after systemic therapy is feasible, with acceptable morbidity. Predictive factors for long-term outcome include pulmonary metastases and sNED. Future work evaluating treatments that can convert patients into surgical candidates will increase the cure rate of patients with mRCC.
Figures

References
-
- Jemal A, Siegel R, Ward E. Cancer statistics 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Fyfe G, Fisher RI, Rosenberg SA. Results of treatment of 255 patients with metastatic renal cell carcinoma who received high-dose recombinant interleukin-2 therapy. J Clin Oncol. 1995;13:688–696. - PubMed
-
- Pyrhonen S, Salminen E, Ruutu M. Prospective randomized trial of interferon alfa-2a plus vinblastine versus vinblastine alone in patients with advanced renal cell cancer. J Clin Oncol. 1999;17:2859–2867. - PubMed
-
- Rini BI, Vogelzang NJ, Dumas MC. Phase II trial of weekly intravenous gemcitabine with continuous infusion fluorouracil in patients with metastatic renal cell cancer. J Clin Oncol. 2000;18:2419–2426. - PubMed
-
- Escudier B, Eisen T, Stadler WM. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007;356:125–134. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
