

Serial PIB and MRI in normal, mild cognitive impairment and Alzheimer's disease: implications for sequence of pathological events in Alzheimer's disease
- PMID: 19339253
- PMCID: PMC2677798
- DOI: 10.1093/brain/awp062
Serial PIB and MRI in normal, mild cognitive impairment and Alzheimer's disease: implications for sequence of pathological events in Alzheimer's disease
Abstract
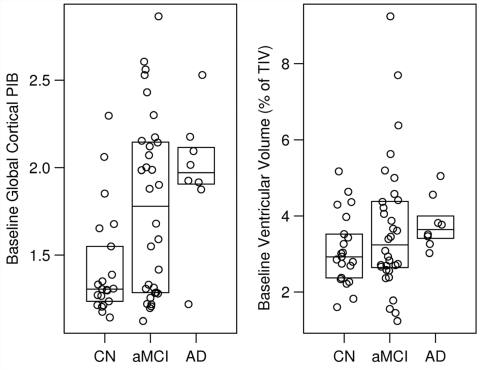
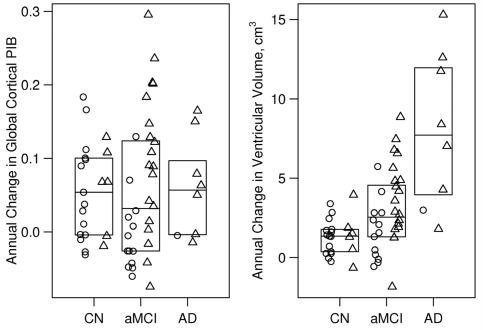
The purpose of this study was to use serial imaging to gain insight into the sequence of pathologic events in Alzheimer's disease, and the clinical features associated with this sequence. We measured change in amyloid deposition over time using serial (11)C Pittsburgh compound B (PIB) positron emission tomography and progression of neurodegeneration using serial structural magnetic resonance imaging. We studied 21 healthy cognitively normal subjects, 32 with amnestic mild cognitive impairment and 8 with Alzheimer's disease. Subjects were drawn from two sources--ongoing longitudinal registries at Mayo Clinic, and the Alzheimer's disease Neuroimaging Initiative (ADNI). All subjects underwent clinical assessments, MRI and PIB studies at two time points, approximately one year apart. PIB retention was quantified in global cortical to cerebellar ratio units and brain atrophy in units of cm(3) by measuring ventricular expansion. The annual change in global PIB retention did not differ by clinical group (P = 0.90), and although small (median 0.042 ratio units/year overall) was greater than zero among all subjects (P < 0.001). Ventricular expansion rates differed by clinical group (P < 0.001) and increased in the following order: cognitively normal (1.3 cm(3)/year) < amnestic mild cognitive impairment (2.5 cm(3)/year) < Alzheimer's disease (7.7 cm(3)/year). Among all subjects there was no correlation between PIB change and concurrent change on CDR-SB (r = -0.01, P = 0.97) but some evidence of a weak correlation with MMSE (r =-0.22, P = 0.09). In contrast, greater rates of ventricular expansion were clearly correlated with worsening concurrent change on CDR-SB (r = 0.42, P < 0.01) and MMSE (r =-0.52, P < 0.01). Our data are consistent with a model of typical late onset Alzheimer's disease that has two main features: (i) dissociation between the rate of amyloid deposition and the rate of neurodegeneration late in life, with amyloid deposition proceeding at a constant slow rate while neurodegeneration accelerates and (ii) clinical symptoms are coupled to neurodegeneration not amyloid deposition. Significant plaque deposition occurs prior to clinical decline. The presence of brain amyloidosis alone is not sufficient to produce cognitive decline, rather, the neurodegenerative component of Alzheimer's disease pathology is the direct substrate of cognitive impairment and the rate of cognitive decline is driven by the rate of neurodegeneration. Neurodegeneration (atrophy on MRI) both precedes and parallels cognitive decline. This model implies a complimentary role for MRI and PIB imaging in Alzheimer's disease, with each reflecting one of the major pathologies, amyloid dysmetabolism and neurodegeneration.
Figures

References
-
- American Psychiatric Association. DSM-IV. Washington, DC: American Psychiatric Association; 1994. Diagnostic and statistical manual of mental disorders.
-
- Andreasen N, Hesse C, Davidsson P, Minthon L, Wallin A, Winblad B, et al. Cerebrospinal fluid beta-amyloid(1-42) in Alzheimer disease: differences between early- and late-onset alzheimer disease and stability during the course of disease. Arch Neurol. 1999;56:673–80. - PubMed
-
- Archer HA, Edison P, Brooks DJ, Barnes J, Frost C, Yeatman T, et al. Amyloid load and cerebral atrophy in Alzheimer's disease: an 11C-PIB positron emission tomography study. Ann Neurol. 2006;60:145–7. - PubMed
-
- Bacskai BJ, Frosch MP, Freeman SH, Raymond SB, Augustinack JC, Johnson KA, et al. Molecular imaging with Pittsburgh Compound B confirmed at autopsy: a case report. Arch Neurol. 2007;64:431–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
