

Blood pressure components and the risk for end-stage renal disease and death in chronic kidney disease
- PMID: 19339424
- PMCID: PMC2666439
- DOI: 10.2215/CJN.06201208
Blood pressure components and the risk for end-stage renal disease and death in chronic kidney disease
Abstract
Background and objectives: Mean arterial pressure has been used in clinical trials in nephrology to randomly assign and treat patients, yet the pulsatile component of BP is recognized to influence outcomes in older people. I examined the unique contributions of systolic (SBP) and diastolic BP (DBP) on the risk for ESRD and death in patients with chronic kidney disease (CKD).
Design, setting, participants, & measurements: A single-center, prospective cohort study was conducted of 218 veterans with CKD (22% black, 4% women, mean age 68 yr, clinic BP 154.1 +/- 25.1/85.2 +/- 13.9 mmHg, 48% with diabetes).
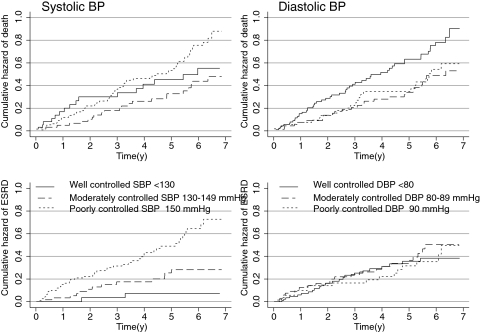
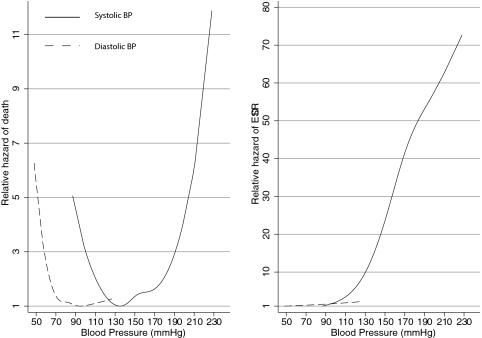
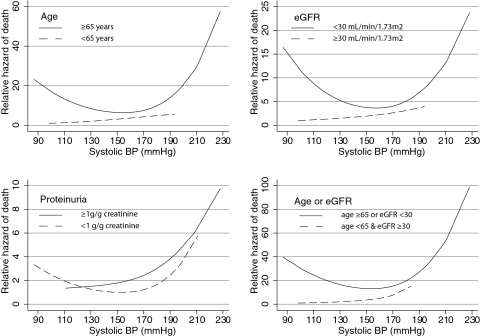
Results: During follow-up of up to 7 yr, 63 patients had ESRD and 102 patients died. Compared with those with controlled SBP (<130 mmHg), patients with moderate control (130 to 149 mmHg) had hazard ratio of 3.87 and those with poor control hazard ratio of 9.09 for ESRD. DBP had no direct ability to predict ESRD. For all-cause mortality, a J-shaped relationship was seen for SBP and an inverse relationship was seen for DBP. Considered jointly in the Cox model, a higher SBP and lower DBP improved the prediction of all-cause mortality compared with either BP component alone. The presence of J curve was especially pronounced in patients with advanced CKD, absence of clinical proteinuria, or age >65 yr.
Conclusions: In older patients with CKD, SBP predicts ESRD and a higher SBP and lower DBP predicts all-cause mortality. Lower BP of <110/70 mmHg is a marker of higher mortality in older individuals with advanced CKD.
Figures
References
-
- Safar ME, Blacher J, Pannier B, Guerin AP, Marchais SJ, Guyonvarc'h PM, London GM: Central pulse pressure and mortality in end-stage renal disease. Hypertension 39: 735–738, 2002 - PubMed
-
- O'Rourke MF: Wave travel and reflection in the arterial system. J Hypertens 17[Suppl 5]: S45–S47, 1999 - PubMed
-
- Agarwal R: Antihypertensive agents and arterial stiffness: Relevance to reducing cardiovascular risk in the chronic kidney disease patient. Curr Opin Nephrol Hypertens 16: 409–415, 2007 - PubMed
-
- Bakris GL, Weir MR, Shanifar S, Zhang Z, Douglas J, van Dijk DJ, Brenner BM: Effects of blood pressure level on progression of diabetic nephropathy: Results from the RENAAL study. Arch Intern Med 163: 1555–1565, 2003 - PubMed
-
- Pohl MA, Blumenthal S, Cordonnier DJ, De AF, DeFerrari G, Eisner G, Esmatjes E, Gilbert RE, Hunsicker LG, de Faria JB, Mangili R, Moore J Jr, Reisin E, Ritz E, Schernthaner G, Spitalewitz S, Tindall H, Rodby RA, Lewis EJ: Independent and additive impact of blood pressure control and angiotensin II receptor blockade on renal outcomes in the irbesartan diabetic nephropathy trial: Clinical implications and limitations. J Am Soc Nephrol 16: 3027–3037, 2005 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
