

Disparities in lupus care and outcomes
- PMID: 19339919
- PMCID: PMC2774141
- DOI: 10.1097/BOR.0b013e328323daad
Disparities in lupus care and outcomes
Abstract
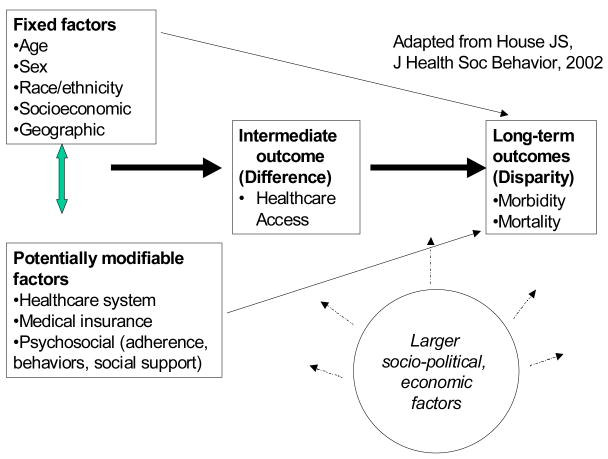
Purpose of review: Systemic lupus erythematosus (SLE), an inflammatory rheumatic disease characterized by autoantibody production and diverse clinical manifestations, disproportionately affects vulnerable groups: women, racial and ethnic minorities, the poor and those lacking medical insurance and education. We summarize the current knowledge of the disparities observed in SLE and highlight recent research that aims to dissect the causes of these disparities and identify the potentially modifiable factors contributing to them.
Recent findings: Several remediable causes, including lack of education, self-efficacy and access to quality, experienced healthcare have been found to contribute to observed disparities in SLE prevalence and outcomes.
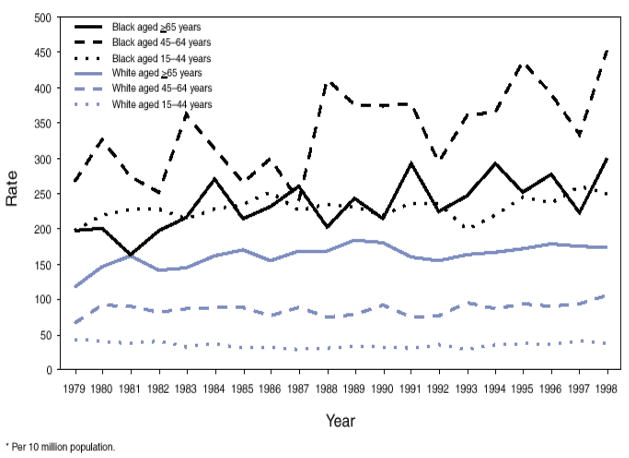
Summary: SLE is associated with alarming disparities in incidence, severity and outcomes. The causes of these disparities are under study by several research groups. Identifying potentially correctable contributory factors should allow the development of effective strategies to improve the healthcare delivery and outcomes in all SLE patients.
Figures
Comment in
-
Clinical research in rheumatology: many promises and several disappointments.Curr Opin Rheumatol. 2009 Mar;21(2):93-4. doi: 10.1097/BOR.0b013e328326791b. Curr Opin Rheumatol. 2009. PMID: 19339917 No abstract available.
References
-
- Sundquist J, Johansson SE. The influence of socioeconomic status, ethnicity and lifestyle on body mass index in a longitudinal study. International journal of epidemiology. 1998;27(1):57–63. - PubMed
-
- Agodoa L, Norris K, Pugsley D. The disproportionate burden of kidney disease in those who can least afford it. Kidney Int Suppl. 2005;(97):S1–3. - PubMed
-
- Shai I, Jiang R, Manson JE, Stampfer MJ, Willett WC, Colditz GA, Hu FB. Ethnicity, obesity, and risk of type 2 diabetes in women: a 20-year follow-up study. Diabetes care. 2006;29(7):1585–90. - PubMed
-
- House JS. Understanding social factors and inequalities in health: 20th century progress and 21st century prospects. Journal of health and social behavior. 2002;43(2):125–42. - PubMed
-
- House JS, Landis KR, Umberson D. Social relationships and health. Science. 1988;241(4865):540–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
