

Intradermal influenza vaccination of healthy adults using a new microinjection system: a 3-year randomised controlled safety and immunogenicity trial
- PMID: 19341446
- PMCID: PMC2676311
- DOI: 10.1186/1741-7015-7-13
Intradermal influenza vaccination of healthy adults using a new microinjection system: a 3-year randomised controlled safety and immunogenicity trial
Abstract
Background: Intradermal vaccination provides direct and potentially more efficient access to the immune system via specialised dendritic cells and draining lymphatic vessels. We investigated the immunogenicity and safety during 3 successive years of different dosages of a trivalent, inactivated, split-virion vaccine against seasonal influenza given intradermally using a microinjection system compared with an intramuscular control vaccine.
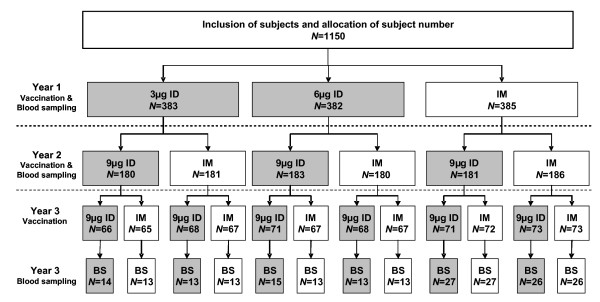
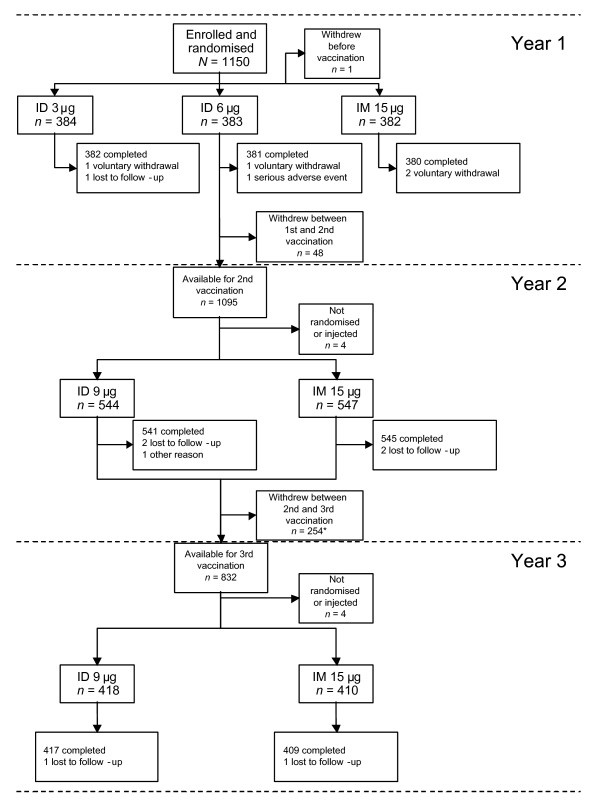
Methods: In a randomised, partially blinded, controlled study, healthy volunteers (1150 aged 18 to 57 years at enrollment) received three annual vaccinations of intradermal or intramuscular vaccine. In Year 1, subjects were randomised to one of three groups: 3 microg or 6 microg haemagglutinin/strain/dose of inactivated influenza vaccine intradermally, or a licensed inactivated influenza vaccine intramuscularly containing 15 microg/strain/dose. In Year 2 subjects were randomised again to one of two groups: 9 microg/strain/dose intradermally or 15 microg intramuscularly. In Year 3 subjects were randomised a third time to one of two groups: 9 microg intradermally or 15 microg intramuscularly. Randomisation lists in Year 1 were stratified for site. Randomisation lists in Years 2 and 3 were stratified for site and by vaccine received in previous years to ensure the inclusion of a comparable number of subjects in a vaccine group at each centre each year. Immunogenicity was assessed 21 days after each vaccination. Safety was assessed throughout the study.
Results: In Years 2 and 3, 9 microg intradermal was comparably immunogenic to 15 microg intramuscular for all strains, and both vaccines met European requirements for annual licensing of influenza vaccines. The 3 microg and 6 microg intradermal formulations were less immunogenic than intramuscular 15 microg. Safety of the intradermal and intramuscular vaccinations was comparable in each year of the study. Injection site erythema and swelling was more common with the intradermal route.
Conclusion: An influenza vaccine with 9 microg of haemagglutinin/strain given using an intradermal microinjection system showed comparable immunogenic and safety profiles to a licensed intramuscular vaccine, and presents a promising alternative to intramuscular vaccination for influenza for adults younger than 60 years.
Trial registration: (Clinicaltrials.gov) NCT00703651.
Figures
Similar articles
-
Intradermal influenza vaccine administered using a new microinjection system produces superior immunogenicity in elderly adults: a randomized controlled trial.J Infect Dis. 2008 Sep 1;198(5):650-8. doi: 10.1086/590434. J Infect Dis. 2008. PMID: 18652550 Clinical Trial.
-
Seasonal influenza vaccine delivered by intradermal microinjection: A randomised controlled safety and immunogenicity trial in adults.Vaccine. 2008 Dec 2;26(51):6614-9. doi: 10.1016/j.vaccine.2008.09.078. Vaccine. 2008. PMID: 18930093 Clinical Trial.
-
Immunogenicity, large scale safety and lot consistency of an intradermal influenza vaccine in adults aged 18-60 years: Randomized, controlled, phase III trial.Hum Vaccin. 2010 Apr;6(4):346-54. doi: 10.4161/hv.6.4.10961. Epub 2010 Apr 15. Hum Vaccin. 2010. PMID: 20372053 Clinical Trial.
-
Fluzone(®) Intradermal vaccine: a promising new chance to increase the acceptability of influenza vaccination in adults.Expert Rev Vaccines. 2012 Jan;11(1):17-25. doi: 10.1586/erv.11.154. Expert Rev Vaccines. 2012. PMID: 22149703 Review.
-
Current evidence on intradermal influenza vaccines administered by Soluvia™ licensed micro injection system.Hum Vaccin Immunother. 2012 Jan;8(1):67-75. doi: 10.4161/hv.8.1.18419. Epub 2012 Jan 1. Hum Vaccin Immunother. 2012. PMID: 22293531 Free PMC article. Review.
Cited by
-
Long-term immunogenicity of the influenza vaccine at reduced intradermal and full intramuscular doses among healthy young adults.Clin Exp Vaccine Res. 2013 Jul;2(2):115-9. doi: 10.7774/cevr.2013.2.2.115. Epub 2013 Jul 3. Clin Exp Vaccine Res. 2013. PMID: 23858402 Free PMC article.
-
Fractional dose of intradermal compared to intramuscular and subcutaneous vaccination - A systematic review and meta-analysis.Travel Med Infect Dis. 2020 Sep-Oct;37:101868. doi: 10.1016/j.tmaid.2020.101868. Epub 2020 Sep 6. Travel Med Infect Dis. 2020. PMID: 32898704 Free PMC article.
-
Influenza vaccines: unmet needs and recent developments.Infect Chemother. 2013 Dec;45(4):375-86. doi: 10.3947/ic.2013.45.4.375. Epub 2013 Dec 27. Infect Chemother. 2013. PMID: 24475351 Free PMC article. Review.
-
Nine μg intradermal influenza vaccine and 15 μg intramuscular influenza vaccine induce similar cellular and humoral immune responses in adults.Hum Vaccin Immunother. 2014;10(9):2713-20. doi: 10.4161/hv.29695. Hum Vaccin Immunother. 2014. PMID: 25483667 Free PMC article. Clinical Trial.
-
Immunosenescence and Challenges of Vaccination against Influenza in the Aging Population.Aging Dis. 2012 Feb;3(1):68-90. Epub 2011 Sep 30. Aging Dis. 2012. PMID: 22500272 Free PMC article.
References
-
- Molinari NA, Ortega-Sanchez IR, Messonnier ML, Thompson WW, Wortley PM, Weintraub E, Bridges CB. The annual impact of seasonal influenza in the US: measuring disease burden and costs. Vaccine. 2007;25:5086–5096. - PubMed
-
- Fiore AE, Shay DK, Haber P, Iskander JK, Uyeki TM, Mootrey G, Bresee JS, Cox NJ, Advisory Committee on Immunization Practices (ACIP) Centers for Disease Control and prevention (CDC) Prevention and control of influenza. Recommendations of the Advisory Committee on Immunization Practices (ACIP), 2007. MMWR Recomm Rep. 2007;56:1–54. - PubMed
-
- van Essen GA, Palache AM, Forleo E, Fedson DS. Influenza vaccination in 2000: recommendations and vaccine use in 50 developed and rapidly developing countries. Vaccine. 2003;21:1780–1785. - PubMed
-
- Scuffham PA, West PA. Economic evaluation of strategies for the control and management of influenza in Europe. Vaccine. 2002;20:2562–2578. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
