

Circumferential strain analysis identifies strata of cardiomyopathy in Duchenne muscular dystrophy: a cardiac magnetic resonance tagging study
- PMID: 19341862
- PMCID: PMC2709409
- DOI: 10.1016/j.jacc.2008.12.032
Circumferential strain analysis identifies strata of cardiomyopathy in Duchenne muscular dystrophy: a cardiac magnetic resonance tagging study
Abstract
Objectives: This study sought to evaluate the natural history of occult cardiac dysfunction in Duchenne muscular dystrophy (DMD).
Background: Duchenne muscular dystrophy is characterized by progressive cardiac dysfunction and myocardial fibrosis late in the disease process. We hypothesized that left ventricular myocardial peak circumferential strain (epsilon(cc)) would decrease in DMD before global systolic functional abnormalities regardless of age or ventricular ejection fraction (EF).
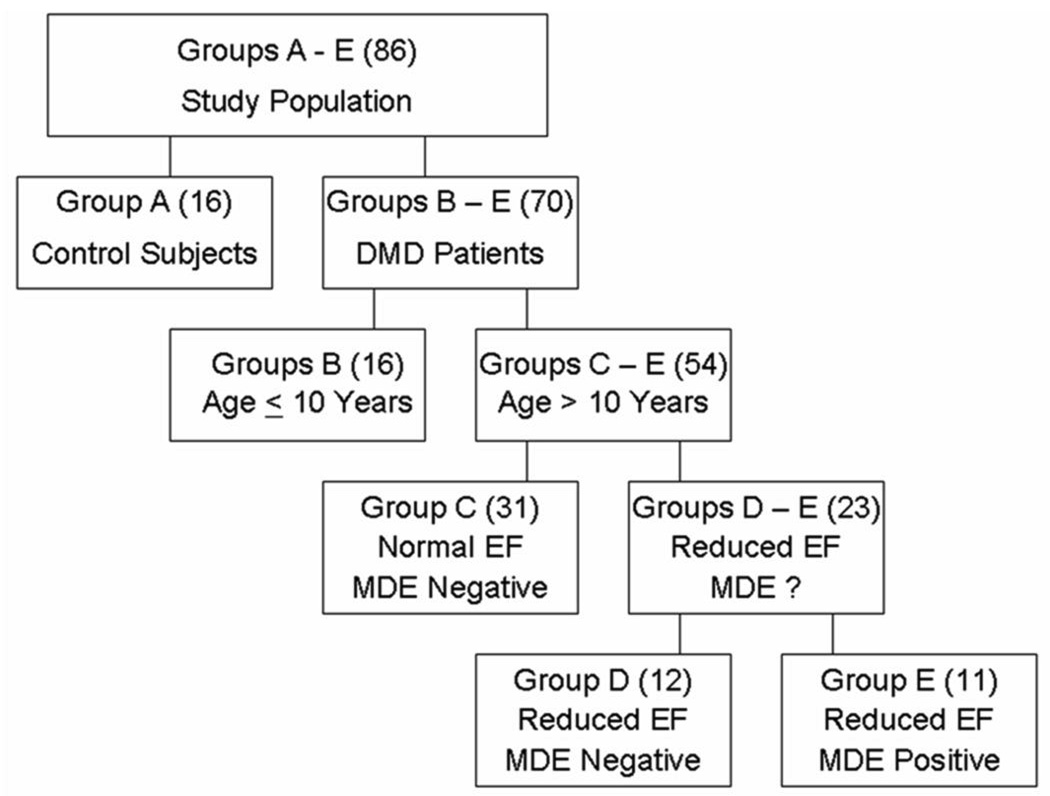
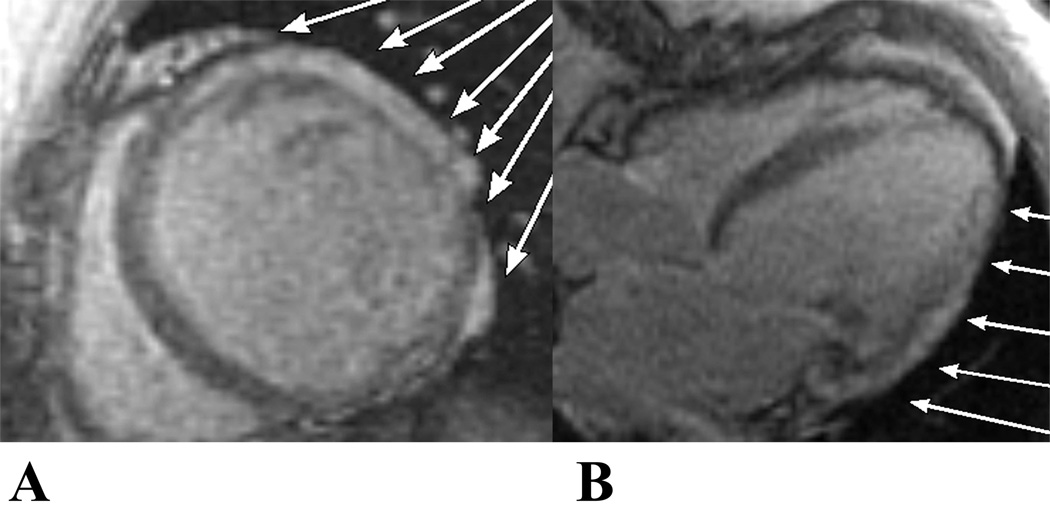
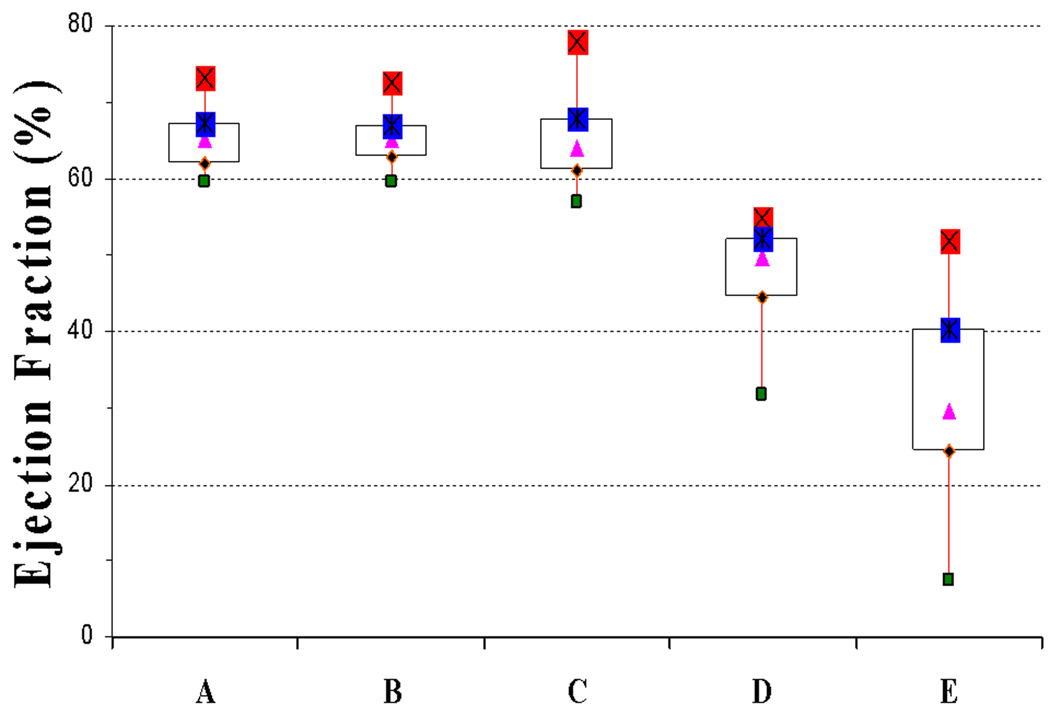
Methods: We evaluated cardiac magnetic resonance image (MRI) data from 70 DMD patients and 16 aged-matched control subjects. Standard imaging data included steady-state free precession short-axis cine stack images, cine myocardial tagged images, and myocardial delayed enhancement (MDE) (an indicator of myocardial fibrosis) sequences. Analysis was performed with QMASS (Medis Medical Imaging Systems, Leiden, the Netherlands) and HARP (Diagnosoft, Palo Alto, California) software. The DMD patient data were subdivided by age (<10 or >10 years), EF (>55% or <55%), and the presence or absence of MDE.
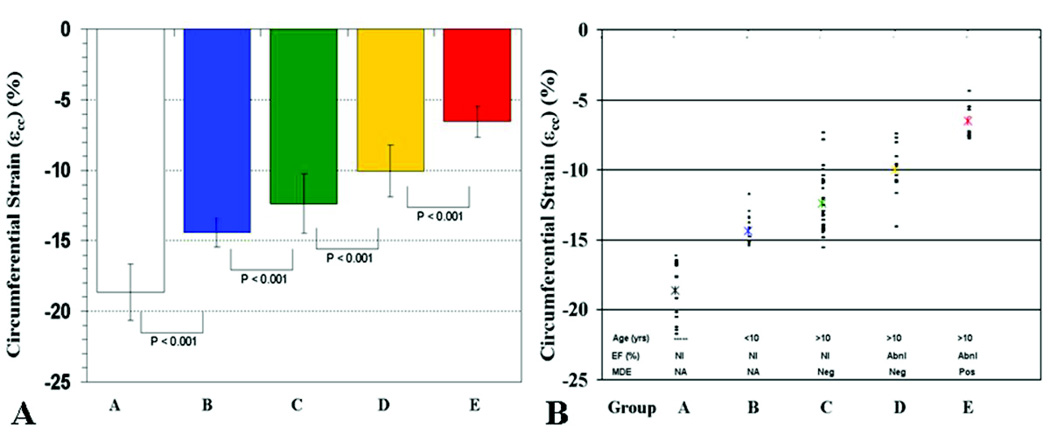
Results: The DMD patients with normal EF had reduced epsilon(cc) at an early age (<10 years) compared with control subjects (p < 0.01). The DMD patients age >10 years with normal EF had further decline in epsilon(cc) compared with younger DMD patients (p < 0.01). There was further decline in epsilon(cc) with age in patients with reduced EF (p < 0.01) without MDE. The oldest patients, with both reduced EF and positive MDE, exhibited the lowest epsilon(cc). None of the patients had ventricular hypertrophy.
Conclusions: Myocardial strain abnormalities are prevalent in young DMD patients despite normal EF, and these strain values continue to decline with advancing age. Strain analysis in combination with standard MRI and MDE imaging provides a means to stratify DMD cardiomyopathy.
Conflict of interest statement
Conflict of Interest and Financial Disclosure: None
Figures

References
-
- McKusick V. Online Mendelian Inheritance in Man, OMIM (TM) Johns Hopkins University; 2005.
-
- de Kermadec JM, Becane HM, Chenard A, Tertrain F, Weiss Y. Prevalence of left ventricular systolic dysfunction in Duchenne muscular dystrophy: an echocardiographic study. Am Heart J. 1994;127:618–623. - PubMed
-
- Angermann C, Spes C, Pongratz D. Cardiac manifestation of progressive muscular dystrophy of the Duchenne type. Z Kardiol. 1986;75:542–551. - PubMed
-
- Moriuchi T, Kagawa N, Mukoyama M, Hizawa K. Autopsy analyses of the muscular dystrophies. Tokushima J Exp Med. 1993;40:83–93. - PubMed
-
- Bushby K, Muntoni F, Urtizberea A, Hughes R, Griggs R. Report on the 124th ENMC International Workshop. Treatment of Duchenne muscular dystrophy; defining the gold standards of management in the use of corticosteroids. 2–4 April 2004, Naarden, The Netherlands. Neuromuscul Disord. 2004;14:526–534. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
