

The Pediatric Cardiomyopathy Registry: 1995-2007
- PMID: 19343086
- PMCID: PMC2408445
- DOI: 10.1016/j.ppedcard.2007.11.006
The Pediatric Cardiomyopathy Registry: 1995-2007
Abstract
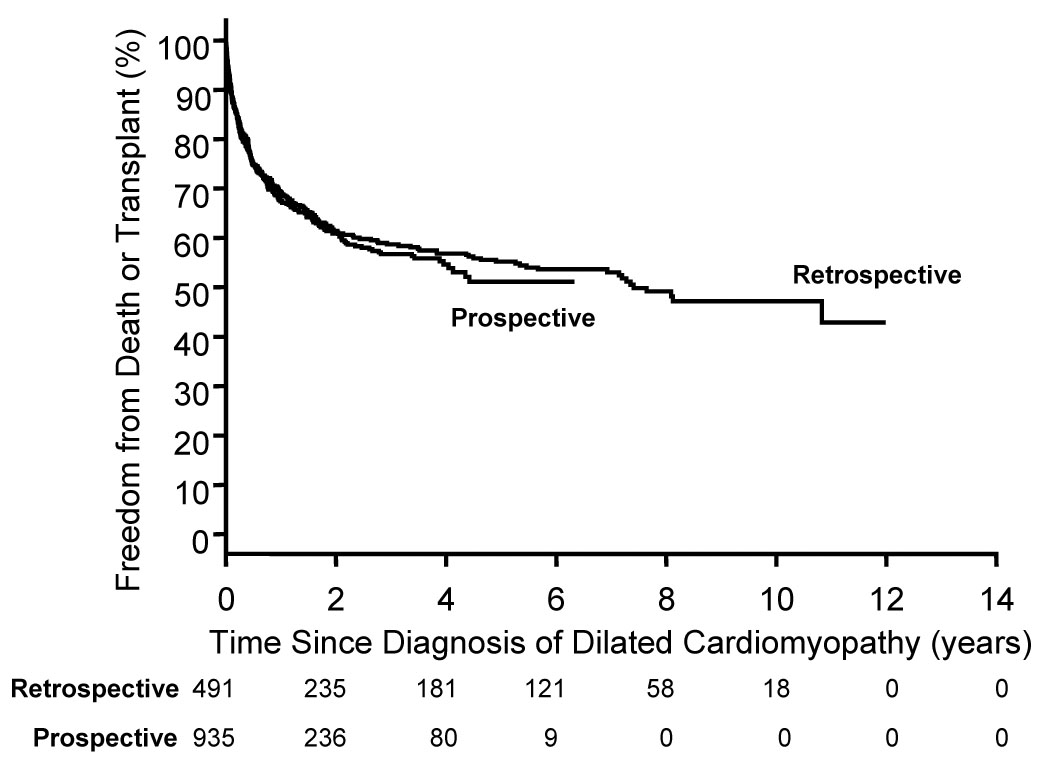
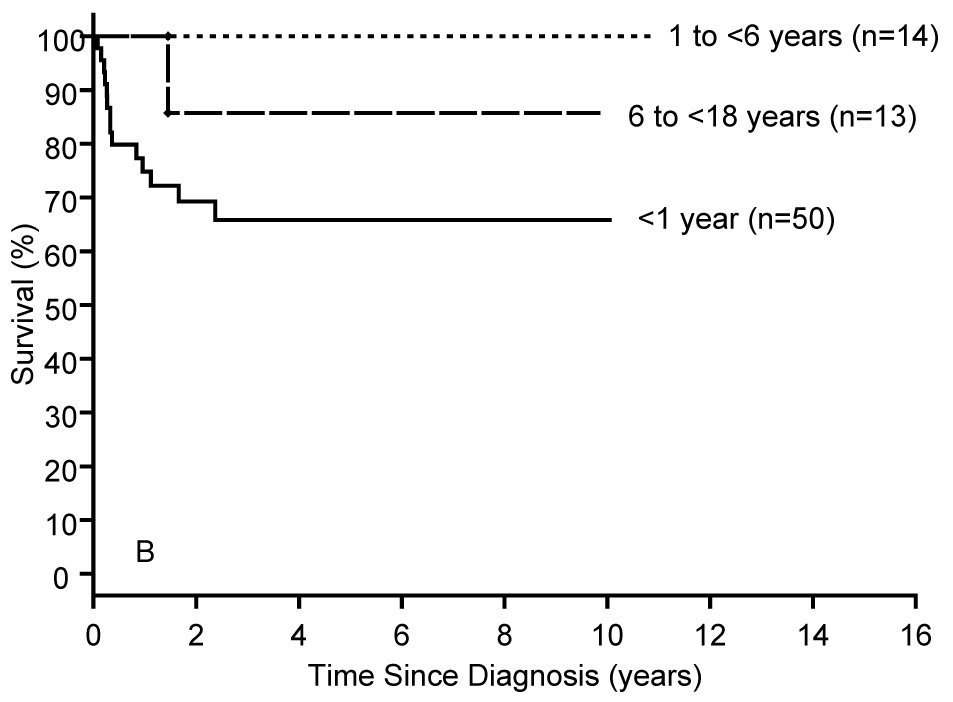
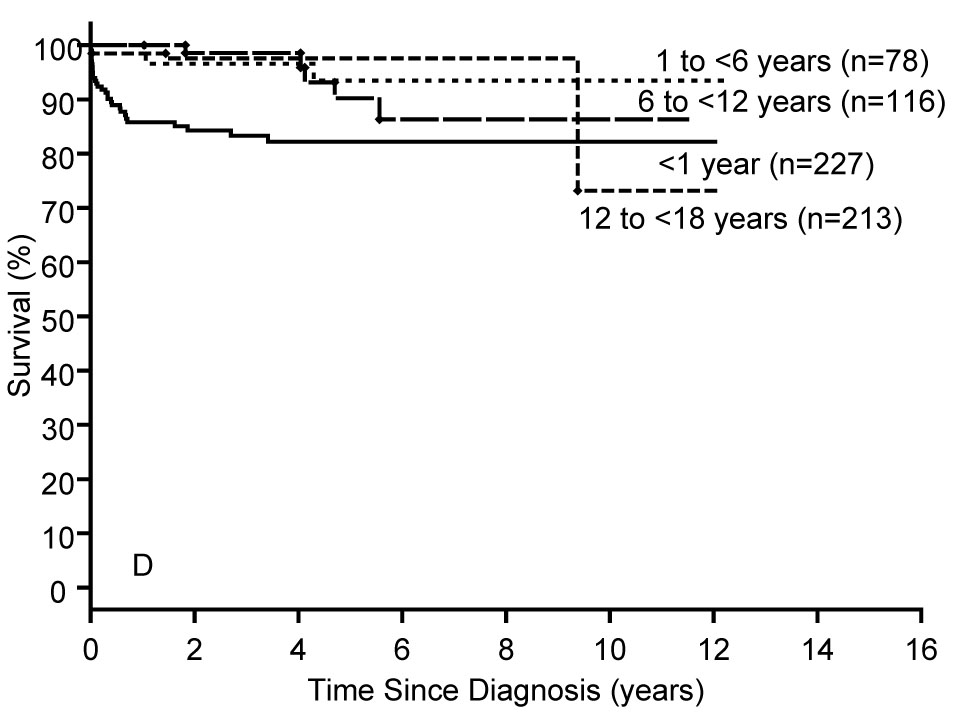
Cardiomyopathy is a serious disorder of the heart muscle and, although rare, it is potentially devastating in children. Funded by the National Heart Lung and Blood Institute since 1994, the Pediatric Cardiomyopathy Registry (PCMR) was designed to describe the epidemiology and clinical course of selected CMs in patients 18 years old or younger and to promote the development of etiology-specific prevention and treatment strategies. Currently, data from more than 3,000 children with cardiomyopathy have been entered in the PCMR database with annual follow-up continuing until death, heart transplant, or loss-to-follow up. Using PCMR data, the incidence of cardiomyopathy in two large regions of the United States is estimated to be 1.13 cases per 100,000 children. Only 1/3 of children had a known etiology at the time of cardiomyopathy diagnosis. Diagnosis was associated with certain patient characteristics, family history, echocardiographic findings, laboratory testing, and biopsy. Greater incidence was found in boys and infants (<1 yr) for both dilated and hypertrophic cardiomyopathy (DCM, HCM) and black race for only DCM. In DCM, prognosis is worse in older children (>1yr), heart failure (HF) at diagnosis or idiopathic etiology. For HCM, worse prognosis is associated with inborn errors of metabolism or combination of HCM and another cardiomyopathy functional type. The best outcomes were observed in children presenting at age >1 yr with idiopathic HCM. PCMR data have enabled analysis of patients with cardiomyopathy and muscular dystrophy, as well as Noonan Syndrome. Currently, collaborations with the Pediatric Heart Transplant Study group and a newly established Pediatric Cardiomyopathy Biologic Specimen Repository at Texas Children's Hospital will continue to yield important results. The PCMR is the largest and most complete multi-center prospective data resource regarding the etiology, clinical course and outcomes for children with cardiomyopathy.
Figures



References
-
- Grenier MA, Osganian SK, Cox GF, et al. Design and implementation of the North American Pediatric Cardiomyopathy Registry. American Heart Journal. 2000;139:S86–S95. - PubMed
-
- Towbin JA, Lowe AM, Colan SD, et al. Incidence, causes, and outcomes of dilated cardiomyopathy in children. Jama. 2006;296:1867–1876. - PubMed
-
- Lipshultz SE, Sleeper LA, Towbin JA, et al. The incidence of pediatric cardiomyopathy in two regions of the United States. N Engl J Med. 2003;348:1647–1655. - PubMed
-
- Arola A, Jokinen E, Ruuskanen O, et al. Epidemiology of idiopathic cardiomyopathies in children and adolescents. A nationwide study in Finland. Am J Epidemiol. 1997;146:385–393. - PubMed
-
- Nugent AW, Daubeney PEF, Chondros P, et al. The epidemiology of childhood cardiomyopathy in Australia. N Engl J Med. 2003;348:1639–1646. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous