

Laparoscopic completely extraperitoneal repair of inguinal hernia in children: a single-institute experience with 1,257 repairs compared with cut-down herniorrhaphy
- PMID: 19343444
- PMCID: PMC2710496
- DOI: 10.1007/s00464-008-0300-7
Laparoscopic completely extraperitoneal repair of inguinal hernia in children: a single-institute experience with 1,257 repairs compared with cut-down herniorrhaphy
Abstract
Background: Conventional open herniorrhaphy in children has been reported to have 0.3-3.8% recurrence and 5.6-30% postoperative contralateral hernia rates. We developed a unique technique to achieve completely extraperitoneal ligation of PPV without any skip areas under laparoscopic control. This report introduces our technique and results compared with the cut-down herniorrhaphy.
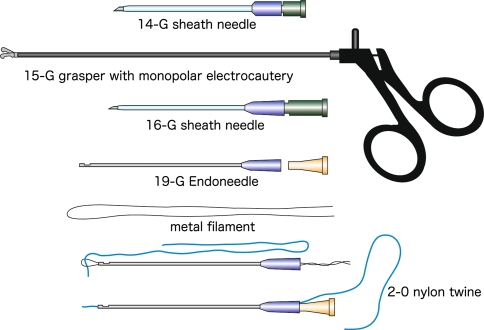
Methods: A consecutive series of 1,585 children with inguinal hernia/hydrocele (1996-2006) was analyzed. In laparoscopic patent processus vaginalis (PPV) closure (LPC), an orifice of PPV was encircled with a 2-0 suture extraperitoneally by a specially devised Endoneedle and tied up from outside of the body achieving completely extraperitoneal ligation of the ring. The round ligament was included in the ligation, whereas the spermatic cord and testicular vessels were excluded by advancing the needle across them behind the peritoneum. Cut-down herniorrhaphy (CD), with or without diagnostic laparoscopy, or LPC was selected according to parental preference under informed consent.
Results: Parents gave more preference to LPC (LPC in 1,257 children, CD in 308, and miscellaneous in 20). Age ranges were equal for both groups. Sex distribution showed female preponderance in the LPC group (44.8% vs. 26.6%, p < 0.001) and umbilical hernia/cysts were predominantly included in the LPC group (11.9% vs. 2.9%, p < 0.001). Mean operation times were equal for both groups for unilateral repair (28.2 +/- 9.2 for LPC vs. 27.8 +/- 13.5 for CD) and were shorter for bilateral repair in the LPC group (35.8 +/- 11.6 vs. 46.7 +/- 17.7). The incidence of postoperative hernia recurrence and contralateral hernia in the LPC group was 0.2% and 0.8%. Two children in the CD group had injuries to their reproductive system during the operation (0.6%).
Conclusions: The advantages of our technique include following: technically simple, short operation time, inspection of bilateral IIRs with simultaneous closure of cPPV, reproductive systems remain intact, routine addition of umbilicoplasty if desired, and essentially indiscernible wounds.
Figures



References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PMC', 'value': 'PMC1616775', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC1616775/'}, {'type': 'PubMed', 'value': '15433221', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15433221/'}]}
- Potts WJ, Riker WL, Lewis JE (1950) The treatment of inguinal hernia in infants and children. Ann Surg 132:566–576 - PMC - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '8497795', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8497795/'}]}
- Skinney MA, Grosfeld JL (1993) Inguinal and umbilical hernia repair in infants and children. Surg Clin North Am 73:439–449 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '6613466', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/6613466/'}]}
- Ingimarsson O, Spak I (1983) Inguinal and femoral hernias: long-term results in a community hospital. Acta Chir Scand 149:291–297 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '5129914', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/5129914/'}]}
- Rowe MI, Clatworthy HW (1971) The other side of the pediatric inguinal hernia. Surg Clin North Am 51:1371–1376 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1053/jpsu.2001.25760', 'is_inner': False, 'url': 'https://doi.org/10.1053/jpsu.2001.25760'}, {'type': 'PubMed', 'value': '11479854', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11479854/'}]}
- Burd RS, Heffington SH, Teague JL (2001) The optimal approach for management of metachronous hernias in children: a decision analysis. J Pediatr Surg 36:1190–1995 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
