

Is passive immunization for Alzheimer's disease 'alive and well' or 'dead and buried'?
- PMID: 19344284
- PMCID: PMC2704502
- DOI: 10.1517/14712590902828285
Is passive immunization for Alzheimer's disease 'alive and well' or 'dead and buried'?
Abstract
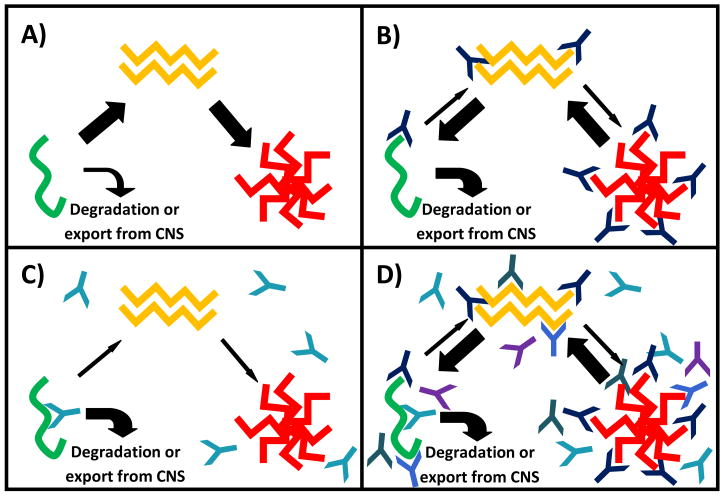
Background: Passive immunization strategies are under investigation as potential disease-modifying therapies for Alzheimer's disease (AD). Current approaches, based on data demonstrating behavioral improvement and reduced pathology in transgenic animal models, have focused exclusively on immune targeting of beta-amyloid.
Objective: To examine immunization strategies for AD.
Methods: A review of relevant publications.
Results/conclusions: Preliminary results from three Phase II trials suggest both the promise and the need to exercise caution with this method of immunotherapy. The strategies used were distinct, using monoclonal N-terminal, central epitope, and polyclonal antibodies to maximize the efficacy and safety of each approach. The tested compounds are moving into Phase III trials for mild to moderate AD. We await the discoveries that from these studies that may yield the first disease-modifying therapy for AD.
Figures
References
-
- Geylis V, Steinitz M. Immunotherapy of Alzheimer’s disease (AD): from murine models to anti-amyloid beta (Abeta) human monoclonal antibodies. Autoimmun Rev. 2006;5(1):33–9. - PubMed
-
- Hawkes CA, McLaurin J. Immunotherapy as treatment for Alzheimer’s disease. Expert Rev Neurother. 2007;7(11):1535–48. - PubMed
-
- Hock C, et al. Antibodies against beta-amyloid slow cognitive decline in Alzheimer’s disease. Neuron. 2003;38(4):547–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical