

Effects of steroids on reintubation and post-extubation stridor in adults: meta-analysis of randomised controlled trials
- PMID: 19344515
- PMCID: PMC2689493
- DOI: 10.1186/cc7772
Effects of steroids on reintubation and post-extubation stridor in adults: meta-analysis of randomised controlled trials
Abstract
Introduction: The efficacy of steroid administration before planned tracheal extubation in critical care patients remains controversial with respect to the selection of patients most likely to benefit from this treatment.
Methods: We performed an extensive literature search for adult trials testing steroids versus placebo to prevent reintubation or laryngeal dyspnoea. Studies were evaluated on a five-point scale based on randomisation, double-blinding and follow-up. Our analysis included trials having a score three or higher with patients mechanically ventilated for at least 24 hours and treated with steroids before extubation, taking into account the time of their administration (early vs late) and if the population selected was at risk or not.
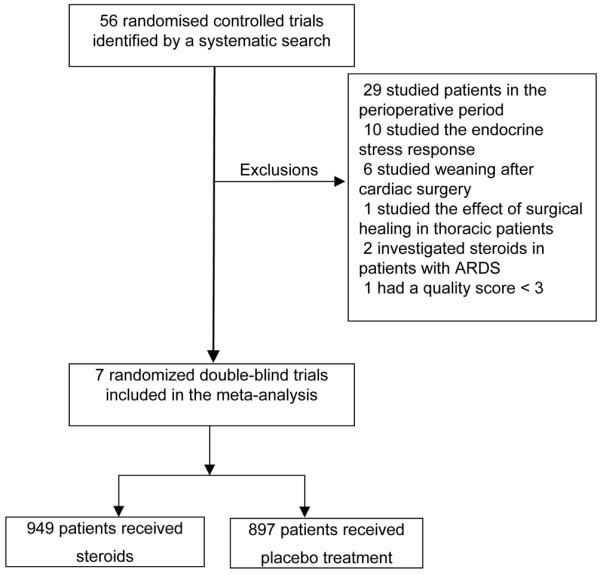
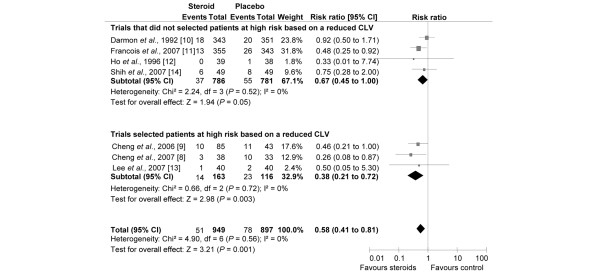
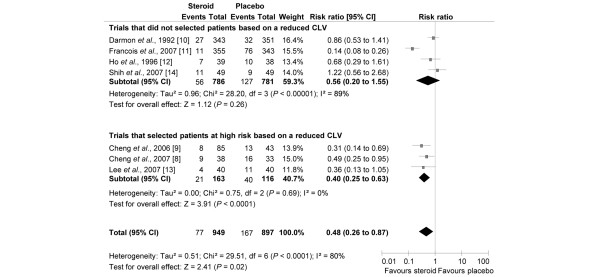
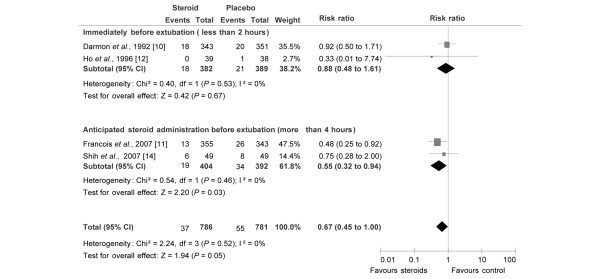
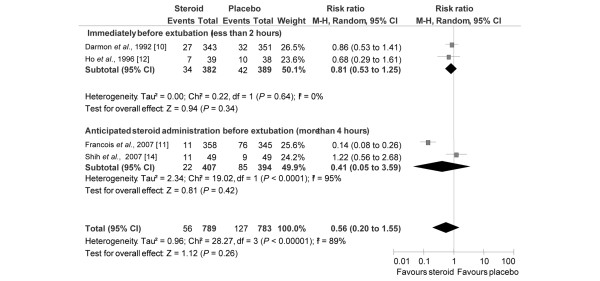
Results: Seven prospective, randomised, double-blinded trials, including 1846 patients, (949 of which received steroids) were selected. Overall, steroids significantly decreased the risk of reintubation (relative risk (RR) = 0.58, 95% confidence interval (CI) = 0.41 to 0.81; number-needed-to-treat (NNT) = 28, 95% CI = 20 to 61) and stridor (RR = 0.48, 95% CI = 0.26 to 0.87; NNT = 11, 95% CI = 8 to 42). The effect of steroids on reintubation and stridor was more pronounced for selected high-risk patients, as determined by a reduced cuff leak volume (RR = 0.38, 95% CI = 0.21 to 0.72; NNT = 9, 95% CI = 7 to 19; and RR = 0.40, 95% CI = 0.25 to 0.63; NNT = 5, 95% CI = 4 to 8, respectively). In contrast, steroid benefit was unclear when trials did not select patients for their risk of reintubation (RR = 0.67, 95% CI = 0.45 to 1.00; NNT = 44, 95% CI >/= 26 to infinity) or stridor (RR = 0.56, 95% CI = 0.20 to 1.55).
Conclusions: The efficacy of steroids to prevent stridor and reintubation was only observed in a high-risk population, as identified by the cuff-leak test and when it was administered at least four hours before extubation. The benefit of steroids remains unclear when patients at high risk are not selected.
Figures
References
-
- de Lassence A, Alberti C, Azoulay E, Le_Miere E, Cheval C, Vincent F, Cohen Y, Garrouste-Orgeas M, Adrie C, Troche G, Timsit JF, OUTCOMEREA Study Group Impact of unplanned extubation and reintubation after weaning on nosocomial pneumonia risk in the intensive care unit: a prospective multicenter study. Anesthesiology. 2002;97:148–156. doi: 10.1097/00000542-200207000-00021. - DOI - PubMed
-
- Epstein SK, Ciubotaru RL. Independent effects of etiology of failure and time to reintubation on outcome for patients failing extubation. Am J Respir Crit Care Med. 1998;158:489–493. - PubMed
-
- Jaber S, Amraoui J, Lefrant J, Arich C, Cohendy R, Landreau L, Calvet Y, Capdevila X, Mahamat A, Eledjam J. Clinical practice and risk factors for immediate complications of endotracheal intubation in intensive care unit: a prospective multicenter study. Crit Care Med. 2006;34:2355–2361. doi: 10.1097/01.CCM.0000233879.58720.87. - DOI - PubMed
-
- Jaber S, Chanques G, Matecki S, Ramonatxo M, Vergne C, Souche B, Perrigault PF, Eledjam JJ. Post-extubation stridor in intensive care unit patients. Risk factors evaluation and importance of the cuff-leak test. Intensive Care Med. 2003;29:69–74. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
