

Complications of bariatric surgery: presentation and emergency management--a review
- PMID: 19344551
- PMCID: PMC2749388
- DOI: 10.1308/003588409X392072
Complications of bariatric surgery: presentation and emergency management--a review
Abstract
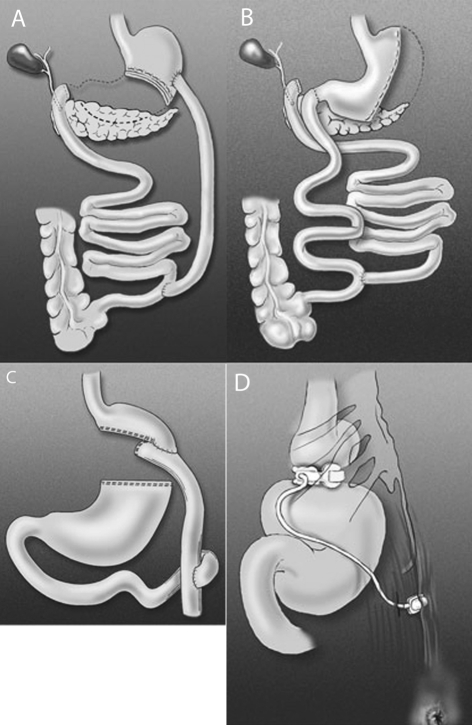
Introduction: The prevalence of obesity surgery is increasing rapidly in the UK as demand rises. Consequently, general surgeons on-call may be faced with the complications of such surgery and need to have an understanding about how to manage them, at least initially. Obesity surgery is mainly offered in tertiary centres but patients may present with problems to their local district hospital. This review summarises the main complications that may be encountered.
Materials and methods: A full literature search was carried out looking at articles published in the last 10 years. Keywords for search purposes included bariatric, surgery, complications, emergency and management.
Conclusions: Complications of bariatric surgery have been extensively written about but never in a format that is designed to aid the on-call surgeon. The intricate details and rare complications have been excluded to concentrate on those symptoms and signs that are likely to be encountered by the emergency team.
Figures


Comment in
-
Comment on: A plethora of gastric bands.Ann R Coll Surg Engl. 2009 Nov;91(8):719; author reply 719. doi: 10.1308/003588409x12486167521433. Ann R Coll Surg Engl. 2009. PMID: 19909618 Free PMC article. No abstract available.
Similar articles
-
Presentation and management of common post-weight loss surgery problems in the emergency department.Ann Emerg Med. 2006 Feb;47(2):160-6. doi: 10.1016/j.annemergmed.2005.06.447. Epub 2005 Aug 15. Ann Emerg Med. 2006. PMID: 16431226 Review.
-
Complications of bariatric surgery.Minerva Chir. 2006 Apr;61(2):125-39. Minerva Chir. 2006. PMID: 16871144 Review.
-
Management of late postoperative complications of bariatric surgery.Br J Surg. 2011 Oct;98(10):1345-55. doi: 10.1002/bjs.7568. Br J Surg. 2011. PMID: 21887775 Review.
-
Role of the gastroenterologist in the management of the obese patient.Gastroenterol Hepatol. 2017 Jun-Jul;40(6):409-416. doi: 10.1016/j.gastrohep.2016.08.001. Epub 2016 Oct 13. Gastroenterol Hepatol. 2017. PMID: 27745965 Review. English, Spanish.
-
BARIATRIC SURGERY IMPACT ON GASTROESOPHAGEAL REFLUX AND DENTAL WEAR: A SYSTEMATIC REVIEW.Arq Bras Cir Dig. 2019 Dec 20;32(4):e1466. doi: 10.1590/0102-672020190001e1466. eCollection 2019. Arq Bras Cir Dig. 2019. PMID: 31859919 Free PMC article.
Cited by
-
Mesentero-axial gastric volvulus after removal of laparoscopic adjustable gastric band.Ann R Coll Surg Engl. 2017 Feb;99(2):e58-e59. doi: 10.1308/rcsann.2016.0313. Epub 2016 Oct 28. Ann R Coll Surg Engl. 2017. PMID: 27791422 Free PMC article.
-
The effect of bariatric surgery on psychiatric course among patients with bipolar disorder.Bipolar Disord. 2013 Nov;15(7):753-63. doi: 10.1111/bdi.12109. Epub 2013 Aug 5. Bipolar Disord. 2013. PMID: 23909994 Free PMC article.
-
Propensity Score Matching Sleeve Gastrectomy vs. Gastric Bypass with 5 Years of Follow-Up.Obes Surg. 2021 Dec;31(12):5156-5165. doi: 10.1007/s11695-021-05706-1. Epub 2021 Sep 13. Obes Surg. 2021. PMID: 34515946
-
Management of Obesity and Obesity-Related Disorders: From Stem Cells and Epigenetics to Its Treatment.Int J Mol Sci. 2023 Jan 24;24(3):2310. doi: 10.3390/ijms24032310. Int J Mol Sci. 2023. PMID: 36768633 Free PMC article. Review.
-
Laparoscopic Gastric Plication versus Laparoscopic Sleeve Gastrectomy: An Up-to-Date Systematic Review and Meta-Analysis.J Obes. 2018 Oct 9;2018:3617458. doi: 10.1155/2018/3617458. eCollection 2018. J Obes. 2018. PMID: 30402281 Free PMC article.
References
-
- Prentice AM. The emerging epidemic of obesity in developing countries. Int J Epidemiol. 2006;35:93–9. - PubMed
-
- Herron DM, Bloomberg R. Complications of bariatric surgery. Minerva Chir. 2006;61:125–39. - PubMed
-
- Singhal R, Kitchen M, Ndrika S, Hunt K, Bridgwater S, Super P. The ‘Birmingham stitch’ – avoiding slippage in laparoscopic gastric banding. Obes Surg. 2008;18:359–63. - PubMed
-
- Arvind N, Bates SE, Morgan JD, Hewin DF, Frering VM, Norton SA. Fixation of the access-port is not required. Obes Surg. 2007;17:577–80. - PubMed
-
- Biagini J, Karam L. Ten years experience with laparoscopic adjustable gastric banding. Obes Surg. 2008;18:573–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous