

Lyme neuroborreliosis: manifestations of a rapidly emerging zoonosis
- PMID: 19346313
- PMCID: PMC7051319
- DOI: 10.3174/ajnr.A1579
Lyme neuroborreliosis: manifestations of a rapidly emerging zoonosis
Abstract
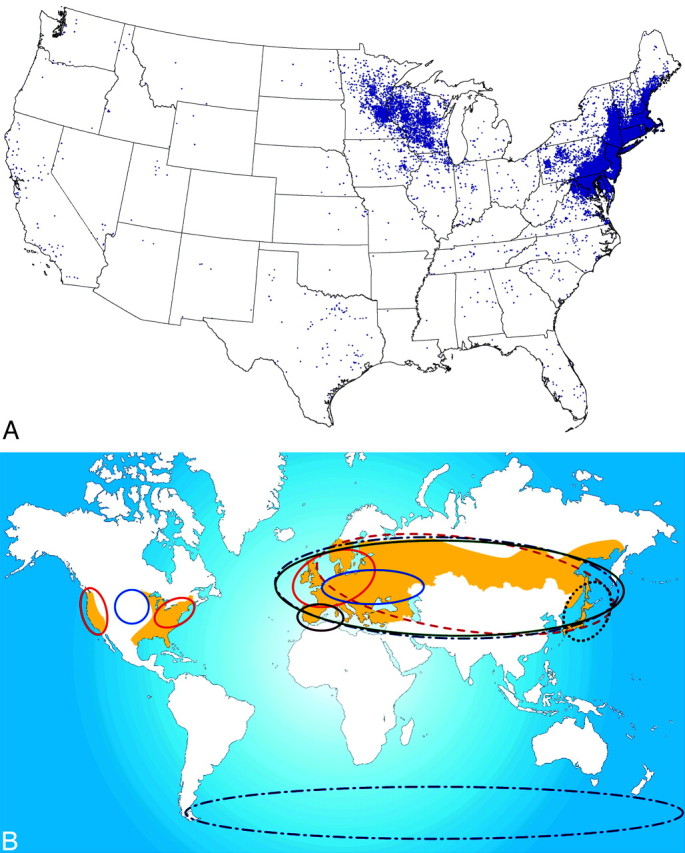
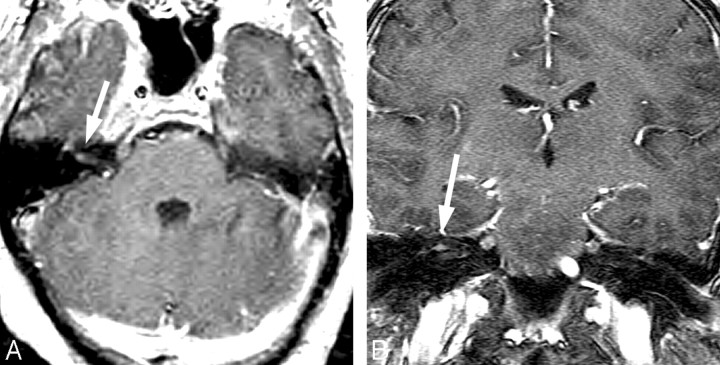
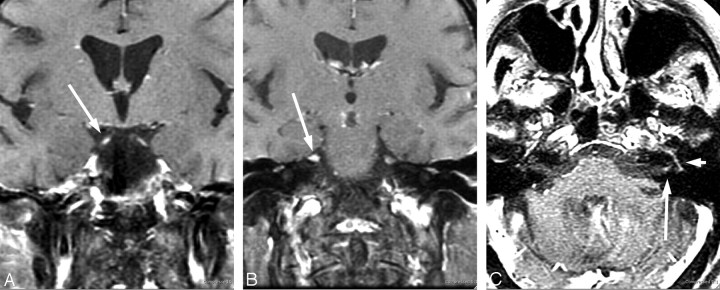
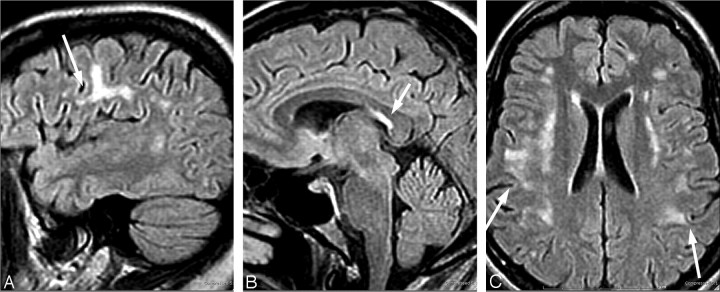
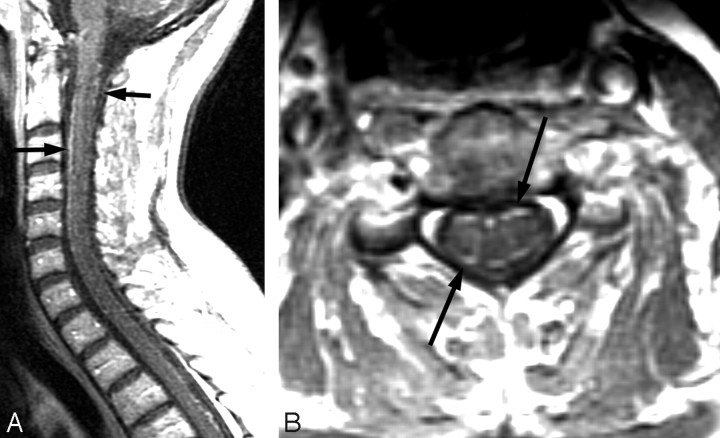
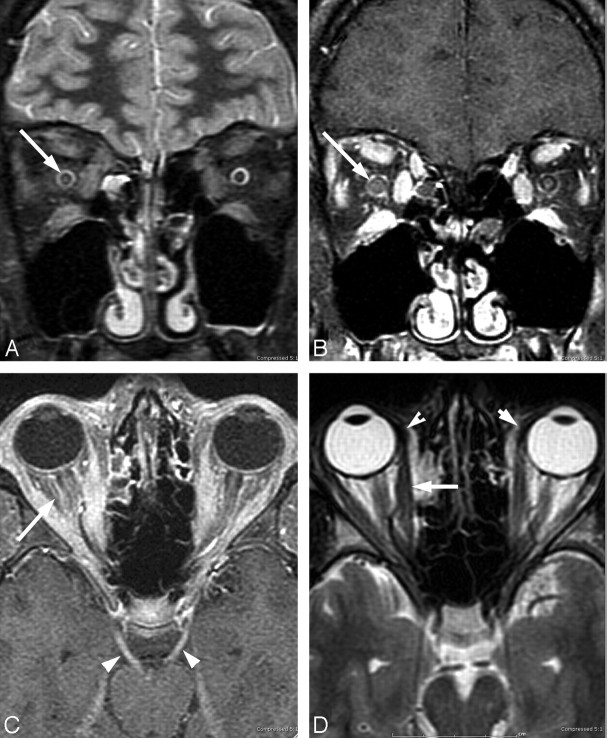
Lyme disease has a worldwide distribution and is the most common vector-borne disease in the United States. Incidence, clinical manifestations, and presentations vary by geography, season, and recreational habits. Lyme neuroborreliosis (LNB) is neurologic involvement secondary to systemic infection by the spirochete Borrelia burgdorferi in the United States and by Borrelia garinii or Borrelia afzelii species in Europe. Enhanced awareness of the clinical presentation of Lyme disease allows inclusion of LNB in the imaging differential diagnosis of facial neuritis, multiple enhancing cranial nerves, enhancing noncompressive radiculitis, and pediatric leptomeningitis with white matter hyperintensities on MR imaging. The MR imaging white matter appearance of successfully treated LNB and multiple sclerosis display sufficient similarity to suggest a common autoimmune pathogenesis for both. This review highlights differences in the epidemiology, clinical manifestations, diagnosis, and management of Lyme disease in the United States, Europe, and Asia, with an emphasis on neurologic manifestations and neuroimaging.
Figures



References
-
- Aberer E. Lyme borreliosis: an update [in English, German]. J Dtsch Dermatol Ges 2007;5:406–14 - PubMed
-
- Jensenius M, Parola P, Raoult D. Threats to international travellers posed by tick-borne diseases. Travel Med Infect Dis 2006;4:4–13. Epub 2004 Dec 20 - PubMed
-
- Centers for Disease Control and Prevention (CDC). Lyme disease: United States, 2003–2005. MMWR Morb Mortal Wkly Rep 2007;56:573–76 - PubMed
-
- Mast WE, Burrows WM, Jr. Erythema chronicum migrans in the United States. JAMA 1976;236:859–60 - PubMed
-
- Mast WE, Burrows WM. Erythema chronicum migrans and “lyme arthritis.” JAMA 1976;236:2392 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical