

Fibrillar amyloid-beta burden in cognitively normal people at 3 levels of genetic risk for Alzheimer's disease
- PMID: 19346482
- PMCID: PMC2665196
- DOI: 10.1073/pnas.0900345106
Fibrillar amyloid-beta burden in cognitively normal people at 3 levels of genetic risk for Alzheimer's disease
Abstract
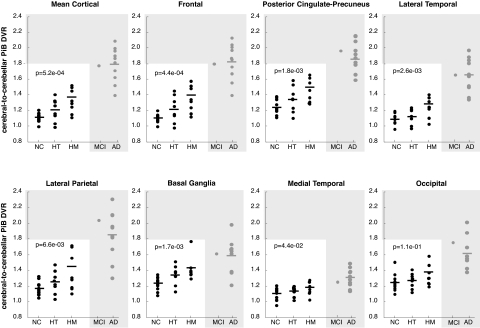
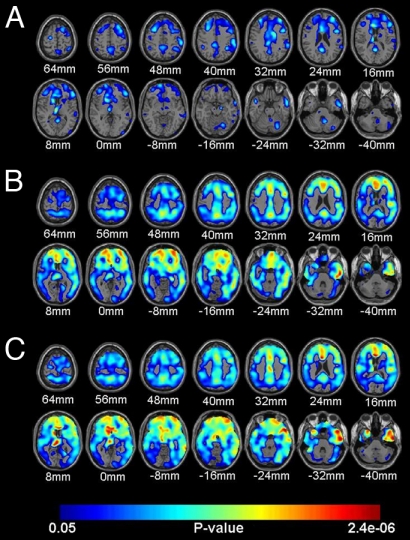
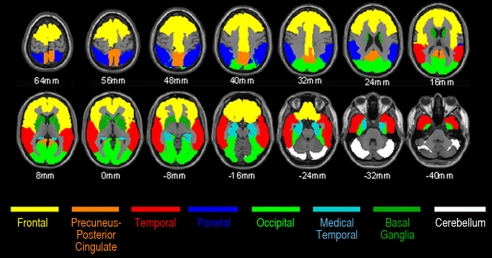
Fibrillar amyloid-beta (Abeta) is found in the brains of many cognitively normal older people. Whether or not this reflects a predisposition to Alzheimer's disease (AD) is unknown. We used Pittsburgh Compound B (PiB) PET to characterize the relationship between fibrillar Abeta burden and this predisposition in cognitively normal older people at 3 mean levels of genetic risk for AD. Dynamic PiB PET scans, the Logan method, statistical parametric mapping, and automatically labeled regions of interest (ROIs) were used to characterize and compare cerebral-to-cerebellar PIB distribution volume ratios, reflecting fibrillar Abeta burden, in 28 cognitively normal persons (mean age, 64 years) with a reported family history of AD and 2 copies, 1 copy, and no copies of the apolipoprotein E (APOE) epsilon4 allele. The 8 epsilon4 homozygotes, 8 heterozygotes, and 12 noncarriers did not differ significantly in terms of age, sex, or cognitive scores. Fibrillar Abeta was significantly associated with APOE epsilon4 carrier status and epsilon4 gene dose in AD-affected mean cortical, frontal, temporal, posterior cingulate-precuneus, parietal, and basal ganglia ROIs, and was highest in an additional homozygote who had recently developed mild cognitive impairment. These findings suggest that fibrillar Abeta burden in cognitively normal older people is associated with APOE epsilon4 gene dose, the major genetic risk factor for AD. Additional studies are needed to track fibrillar Abeta accumulation in persons with different kinds and levels of AD risk; to determine the extent to which fibrillar Abeta, alone or in combination with other biomarkers and risk factors, predicts rates of cognitive decline and conversion to clinical AD; and to establish the role of fibrillar Abeta imaging in primary prevention trials.
Conflict of interest statement
Conflict of interest statement: GE Healthcare holds a license agreement with the University of Pittsburgh based on the technology described in this manuscript and may eventually benefit from the results of the study. Drs. Klunk and Mathis are coinventors of PiB and as such have a financial interest in this license agreement. GE Healthcare provided no grant support for this study, did not charge for our use of PiB, and had no role in the design or interpretation of results or preparation of this manuscript. None of the other authors declares any conflicts of interest.
Figures
References
-
- Hardy J, Selkoe DJ. The amyloid hypothesis of Alzheimer's disease: Progress and problems on the road to therapeutics. Science. 2002;297:353–356. - PubMed
-
- Price JL, Morris JC. Tangles and plaques in nondemented aging and “preclinical” Alzheimer's disease. Ann Neurol. 1999;45:358–368. - PubMed
-
- Oddo S, Billings L, Kesslak JP, Cribbs DH, LaFerla FM. Abeta immunotherapy leads to clearance of early, but not late, hyperphosphorylated tau aggregates via the proteasome. Neuron. 2004;43:321–332. - PubMed
-
- Dickson DW, et al. Identification of normal and pathological aging in prospectively studied nondemented elderly humans. Neurobiol Aging. 1992;13:179–189. - PubMed
-
- Bennett DA, et al. Neuropathology of older persons without cognitive impairment from two community-based studies. Neurology. 2006;66:1837–1844. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
