

Review
doi: 10.1016/j.expneurol.2009.03.031.
Epub 2009 Apr 5.
Management of nerve gaps: autografts, allografts, nerve transfers, and end-to-side neurorrhaphy
Affiliations
- PMID: 19348799
- PMCID: PMC2849924
- DOI: 10.1016/j.expneurol.2009.03.031
Item in Clipboard
Review
Management of nerve gaps: autografts, allografts, nerve transfers, and end-to-side neurorrhaphy
Exp Neurol.
2010 May.
No abstract available
Figures
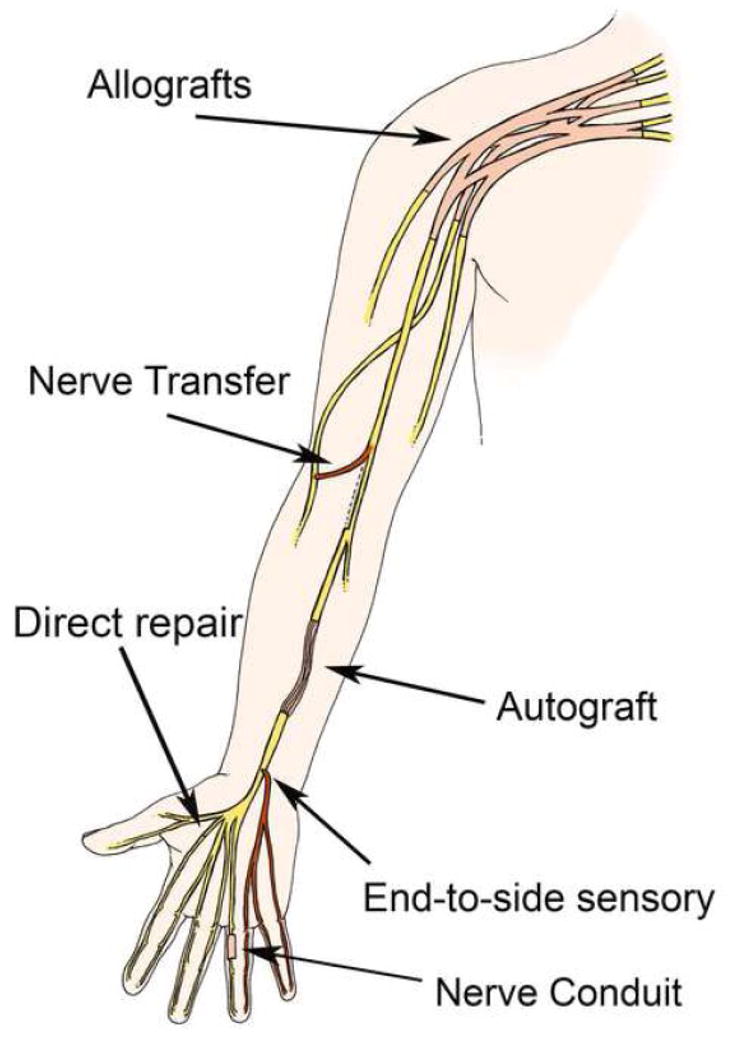
Summarizes the various options for nerve repair. Nerve allografts are utilized for large, otherwise irreparable injuries. Nerve transfer use redundant nerve fibers for a proximal nerve injury. The autograft is used to reconstruct a nerve gap. Direct repair is used when there is no intervening nerve gap to create tension. Both end-to-side and nerve conduits are used for noncritical sensory injuries.
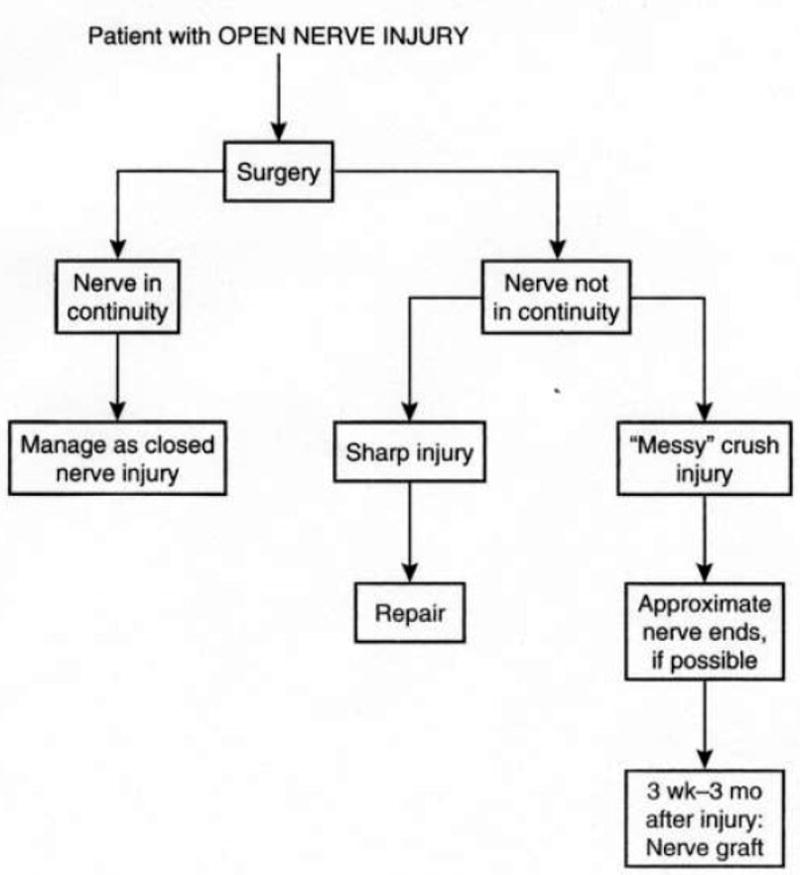
Treatment algorithm for patients with open injuries.

Treatment alorithm for patients with closed injuries.

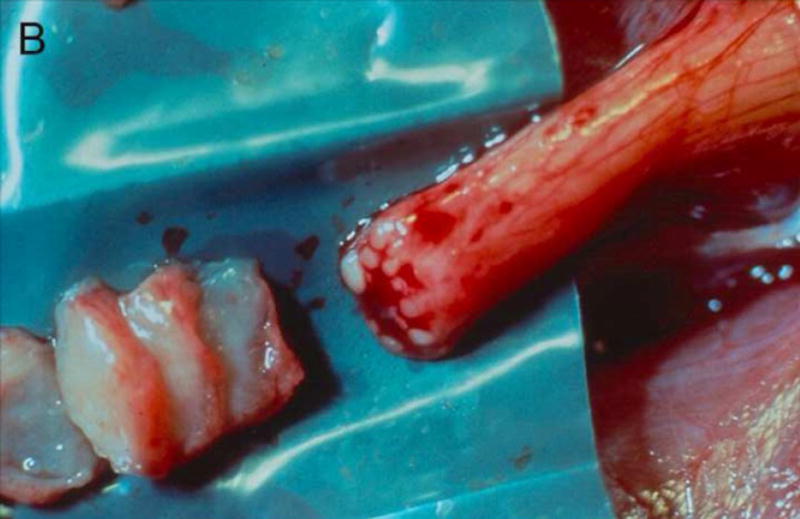
A) Photograph of resected neuroma with disruption of architecture. Sutures are evident from a previous repair, B) Step-wise removal of scar tissue until healthy nerve fascicles are encountered, C) Healthy nerve outside the zone of injury, depicting organized architecture with healthy fascicles prior to nerve grafting. (Images courtesy of Allen Van Beek)
A) Photograph of resected neuroma with disruption of architecture. Sutures are evident from a previous repair, B) Step-wise removal of scar tissue until healthy nerve fascicles are encountered, C) Healthy nerve outside the zone of injury, depicting organized architecture with healthy fascicles prior to nerve grafting. (Images courtesy of Allen Van Beek)

A) Photograph of resected neuroma with disruption of architecture. Sutures are evident from a previous repair, B) Step-wise removal of scar tissue until healthy nerve fascicles are encountered, C) Healthy nerve outside the zone of injury, depicting organized architecture with healthy fascicles prior to nerve grafting. (Images courtesy of Allen Van Beek)

A and C) Illustration of the exposed median and ulnar nerve, the posterior interosseous nerve (PIN) and extensor carpi radialis brevis (ECRB) are depicted in pink and the anterior interosseous nerve (AIN) and flexor digitorum superficialis (FDS) are seen in green, B and D) Median nerve (green) transfer to the radial nerve (pink). (Adapted by permission from Hand Clinics; Elsevier. 2008 Nov; 24(4):319–340, Brown, JM, Mackinnon, SE. Nerve transfers of the forearm and hand)

A and C) Illustration of the exposed median and ulnar nerve, the posterior interosseous nerve (PIN) and extensor carpi radialis brevis (ECRB) are depicted in pink and the anterior interosseous nerve (AIN) and flexor digitorum superficialis (FDS) are seen in green, B and D) Median nerve (green) transfer to the radial nerve (pink). (Adapted by permission from Hand Clinics; Elsevier. 2008 Nov; 24(4):319–340, Brown, JM, Mackinnon, SE. Nerve transfers of the forearm and hand)

A and C) Illustration and photograph demonstrating the AIN in yellow and the deep motor branch of the ulnar in pink, B and D) Transfer of the AIN (yellow) at the level of the pronator quadratus to the motor branch of the ulnar nerve (pink) (Adapted by permission from Hand Clinics; Elsevier. 2008 Nov; 24(4):319–340, Brown, JM, Mackinnon, SE. Nerve transfers of the forearm and hand)

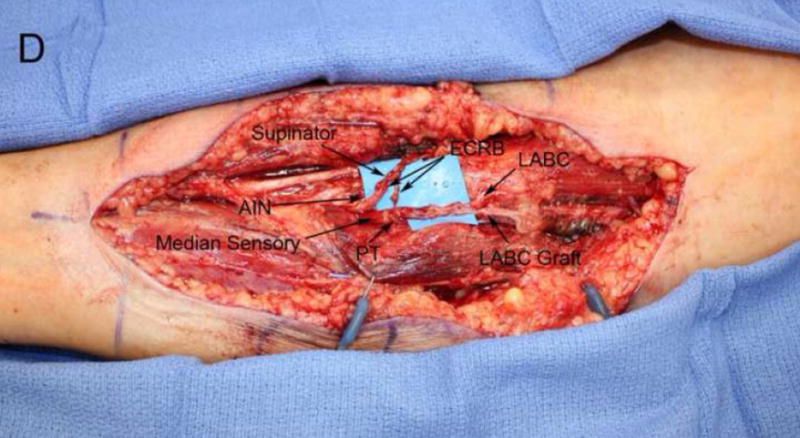
A) Large neuroma in continuity of the proximal median nerve, B) microdissection of the injury and the distal branches, C and D) Illustration and photograph of the finished repair utilizing the LABC as both nerve graft and nerve transfer to the sensory branch of the median nerve, the ECRB was transferred to the PT and the supinator was directed to the AIN. The sensory portion of the median nerve to the 3rd web space was not injuried and was protected.

A) Large neuroma in continuity of the proximal median nerve, B) microdissection of the injury and the distal branches, C and D) Illustration and photograph of the finished repair utilizing the LABC as both nerve graft and nerve transfer to the sensory branch of the median nerve, the ECRB was transferred to the PT and the supinator was directed to the AIN. The sensory portion of the median nerve to the 3rd web space was not injuried and was protected.
A) Large neuroma in continuity of the proximal median nerve, B) microdissection of the injury and the distal branches, C and D) Illustration and photograph of the finished repair utilizing the LABC as both nerve graft and nerve transfer to the sensory branch of the median nerve, the ECRB was transferred to the PT and the supinator was directed to the AIN. The sensory portion of the median nerve to the 3rd web space was not injuried and was protected.

A) Large neuroma in continuity of the proximal median nerve, B) microdissection of the injury and the distal branches, C and D) Illustration and photograph of the finished repair utilizing the LABC as both nerve graft and nerve transfer to the sensory branch of the median nerve, the ECRB was transferred to the PT and the supinator was directed to the AIN. The sensory portion of the median nerve to the 3rd web space was not injuried and was protected.
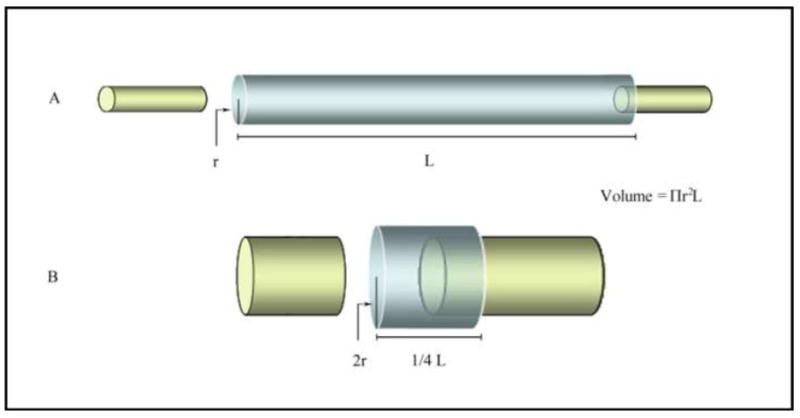
Illustrates the importance of diameter in the volume of a nerve gap. The formula for volume is V = Πr2L, thus doubling the radius (conduit B) requires a length ¼ of conduit A to maintain an equal volume. (Symbols: V = volume, r = radius, Π =pi (~3.14), L = length). (Permission for reproduction from Hand; Springerlink 2009 Jan 10, Epub, Moore, AM et al. Limitations of conduits in peripheral nerve repairs.)

Illustrates the importance of diameter in the volume of a nerve gap. The formula for volume is V = Πr2L, thus doubling the radius (conduit B) requires a length ¼ of conduit A to maintain an equal volume. (Symbols: V = volume, r = radius, Π =pi (~3.14), L = length). (Permission for reproduction from Hand; Springerlink 2009 Jan 10, Epub, Moore, AM et al. Limitations of conduits in peripheral nerve repairs.)
Illustrates the importance of diameter in the volume of a nerve gap. The formula for volume is V = Πr2L, thus doubling the radius (conduit B) requires a length ¼ of conduit A to maintain an equal volume. (Symbols: V = volume, r = radius, Π =pi (~3.14), L = length). (Permission for reproduction from Hand; Springerlink 2009 Jan 10, Epub, Moore, AM et al. Limitations of conduits in peripheral nerve repairs.)
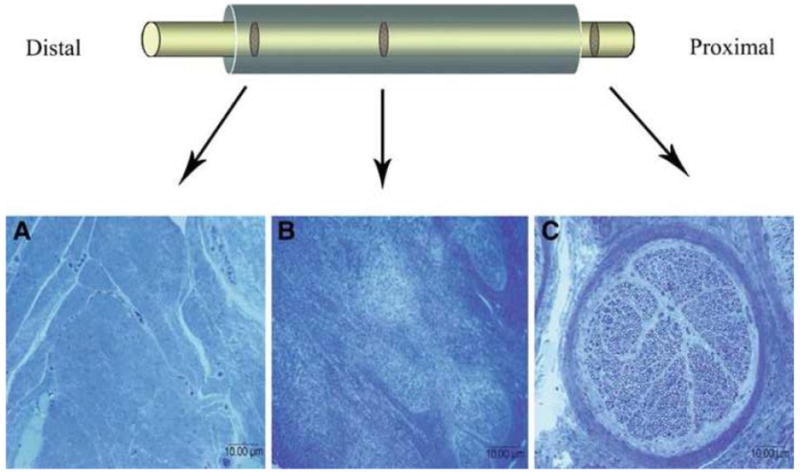
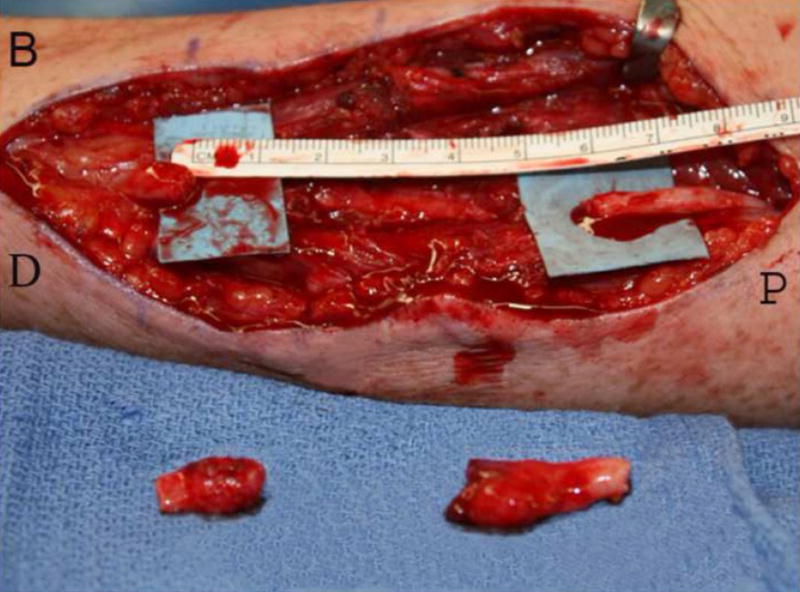
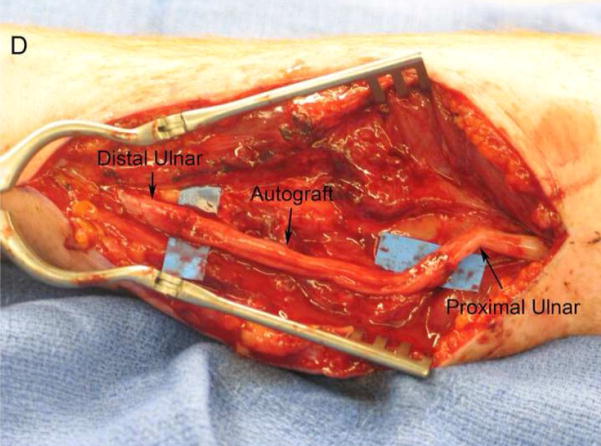
A) Photograph of a large neuroma in continuity following repair with a large PGA nerve conduit, B) The affected segment of nerve was resected leaving a 6 cm nerve gap, C) A- histology of the distal conduit revealed dense fibrinous scar tissue with no discernable nerve structures, B -the mid-conduit section revealed disorganized architecture with no clear axonal organization, C – proximally, normal nerve architecture was demonstrated, D) Photograph of final repair with interposition graft. (Permission for Reproduction from Hand; Springerlink 2009 Jan 10, Epub, Moore, AM et al. Limitations of conduits in peripheral nerve repairs.)
A) Photograph of a large neuroma in continuity following repair with a large PGA nerve conduit, B) The affected segment of nerve was resected leaving a 6 cm nerve gap, C) A- histology of the distal conduit revealed dense fibrinous scar tissue with no discernable nerve structures, B -the mid-conduit section revealed disorganized architecture with no clear axonal organization, C – proximally, normal nerve architecture was demonstrated, D) Photograph of final repair with interposition graft. (Permission for Reproduction from Hand; Springerlink 2009 Jan 10, Epub, Moore, AM et al. Limitations of conduits in peripheral nerve repairs.)
References
-
- Amr SM, Moharram AN. Repair of brachial plexus lesions by end-to-side side-to-side grafting neurorrhaphy: experience based on 11 cases. Microsurgery. 2005;25:126–146. - PubMed
-
- Anderson PN, Turmaine M. Peripheral nerve regeneration through grafts of living and freeze-dried CNS tissue. Neuropathol Appl Neurobiol. 1986;12:389–399. - PubMed
-
- Beaulieu JY, Blustajn J, Teboul F, Baud P, De Schonen S, Thiebaud JB, Oberlin C. Cerebral plasticity in crossed C7 grafts of the brachial plexus: an fMRI study. Microsurgery. 2006;26:303–310. - PubMed
-
- Bertelli JA, Ghizoni MF. Nerve repair by end-to-side coaptation or fascicular transfer: a clinical study. J Reconstr Microsurg. 2003;19:313–318. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
