Comparative study of imaging at 3.0 T versus 1.5 T of the knee
- PMID: 19350234
- PMCID: PMC2704948
- DOI: 10.1007/s00256-009-0683-0
Comparative study of imaging at 3.0 T versus 1.5 T of the knee
Abstract
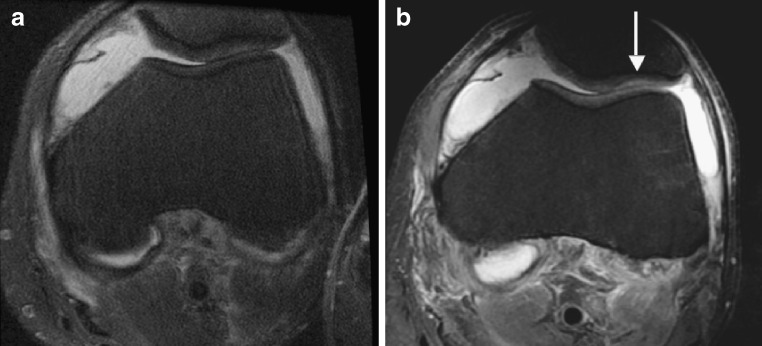
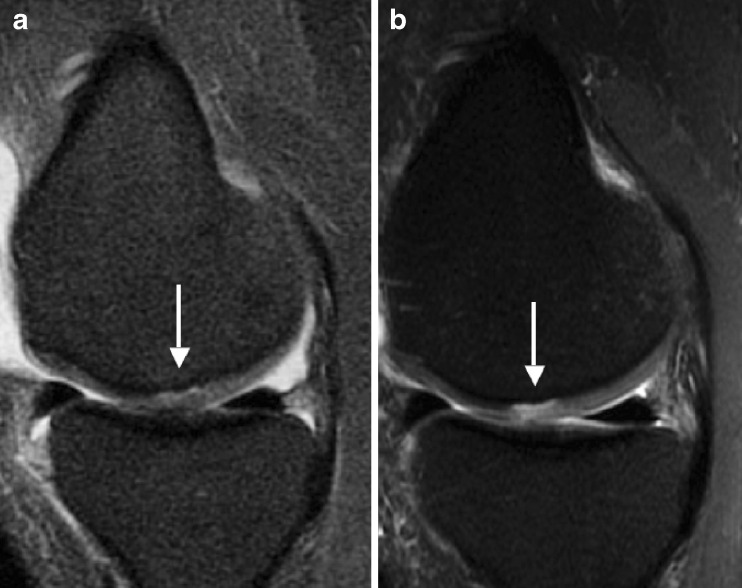
Purpose: The objectives of the study were to compare MR imaging at 1.5 and 3.0 T in the same patients concerning image quality and visualization of cartilage pathology and to assess diagnostic performance using arthroscopy as a standard of reference.
Materials and methods: Twenty-six patients were identified retrospectively as having comparative 1.5 and 3.0 T MR studies of the knee within an average of 102 days. Standard protocols included T1-weighted and fat-saturated intermediate-weighted fast spin-echo sequences in three planes; sequence parameters had been adjusted to account for differences in relaxation at 3.0 T. Arthroscopy was performed in 19 patients. Four radiologists reviewed each study independently, scored image quality, and analyzed pathological findings. Sensitivities, specificities, and accuracies in diagnosing cartilage lesions were calculated in the 19 patients with arthroscopy, and differences between 1.5 and 3.0 T exams were compared using paired Student's t tests with a significance threshold of p < 0.05.
Results: Each radiologist scored the 3.0 T studies higher than those obtained at 1.5 T in visualizing anatomical structures and abnormalities (p < 0.05). Using arthroscopy as a standard of reference, diagnosis of cartilage abnormalities was improved at 3.0 T with higher sensitivity (75.7% versus 70.6%), accuracy (88.2% versus 86.4%), and correct grading of cartilage lesions (51.3% versus 42.9%). Diagnostic confidence scores were higher at 3.0 than 1.5 T (p < 0.05) and signal-to-noise ratio at 3.0 T was approximately twofold higher than at 1.5 T.
Conclusion: MRI at 3.0 T improved visualization of anatomical structures and improved diagnostic confidence compared to 1.5 T. This resulted in significantly better sensitivity and grading of cartilage lesions at the knee.
Figures