

Associations of major bleeding and myocardial infarction with the incidence and timing of mortality in patients presenting with non-ST-elevation acute coronary syndromes: a risk model from the ACUITY trial
- PMID: 19351691
- PMCID: PMC2695951
- DOI: 10.1093/eurheartj/ehp110
Associations of major bleeding and myocardial infarction with the incidence and timing of mortality in patients presenting with non-ST-elevation acute coronary syndromes: a risk model from the ACUITY trial
Abstract
Aims: To evaluate the associations of myocardial infarction (MI) and major bleeding with 1-year mortality. Both MI and major bleeding predict 1-year mortality in patients presenting with acute coronary syndrome (ACS). However, the risk of each of these events on the magnitude and timing of mortality has not been well studied.
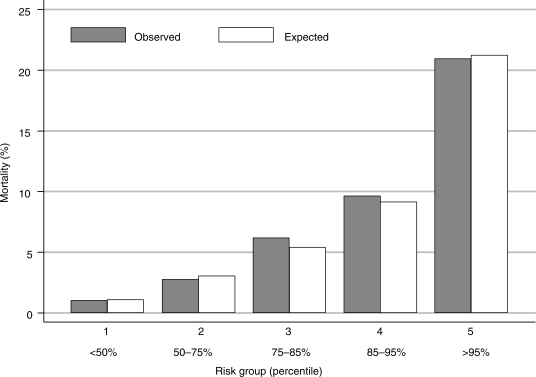
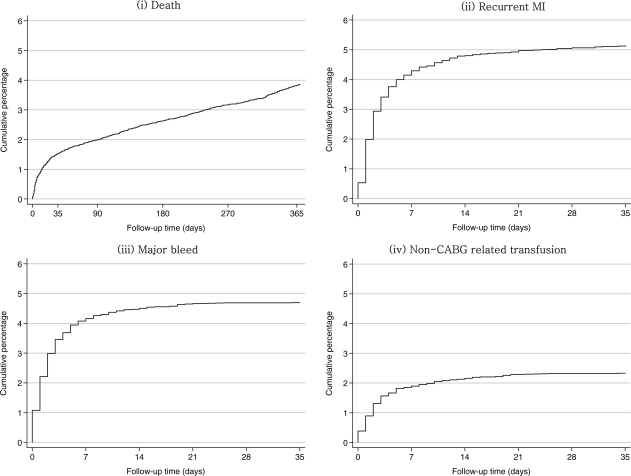
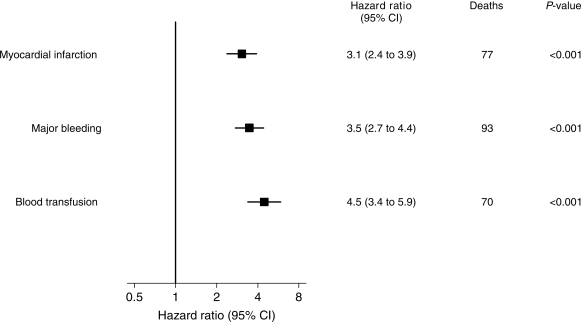
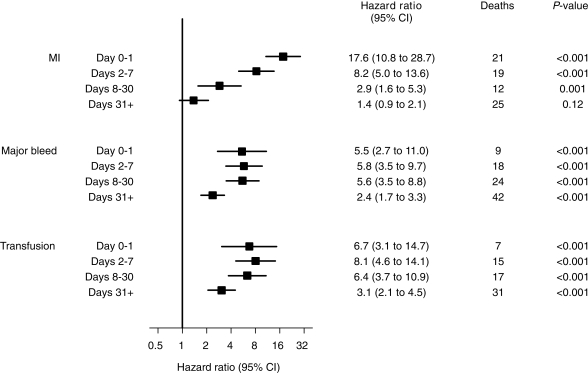
Methods and results: A multivariable Cox regression model was developed relating 13 independent baseline predictors to 1-year mortality for 13 819 patients with moderate and high-risk ACS enrolled in the Acute Catheterization and Urgent Intervention Triage strategy trial. After adjustment for baseline predictors, Cox models with major bleeding and recurrent MI as time-updated covariates estimated the effect of these events on mortality hazard over time. Within 30 days of randomization, 705 patients (5.1%) had an MI, 645 (4.7%) had a major bleed; 524 (3.8%) died within a year. The occurrence of an MI was associated with a hazard ratio of 3.1 compared with patients not yet having an MI, after adjustment for baseline predictors. However, MI within 30 days markedly increased the mortality risk for the first 2 days after the event (adjusted hazard ratio of 17.6), but this risk declined rapidly post-infarct (hazard ratio of 1.4 beyond 1 month after the MI event). In contrast, major bleeding had a prolonged association with mortality risk (hazard ratio of 3.5) which remained fairly steady over time throughout 1 year.
Conclusion: After accounting for baseline predictors of mortality, major bleeds and MI have similar overall strength of association with mortality in the first year after ACS. MI is correlated with a dramatic increase in short-term risk, whereas major bleeding correlates with a more prolonged mortality risk.
Figures
References
-
- Bavry AA, Kumbhani DJ, Rassi AN, Bhatt DL, Askari AT. Benefit of early invasive therapy in acute coronary syndromes: a meta-analysis of contemporary randomized clinical trials. J Am Coll Cardiol. 2006;48:1319–1325. - PubMed
-
- Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS, Jones RH, Kereiakes D, Kupersmith J, Levin TN, Pepine CJ, Schaeffer JW, Smith EE, III, Steward DE, Theroux P, Gibbons RJ, Alpert JS, Faxon DP, Fuster V, Gregoratos G, Hiratzka LF, Jacobs AK, Smith SC, Jr American College of Cardiology; American Heart Association. Committee on the Management of Patients with Unstable Angina. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction—summary article: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on the Management of Patients with Unstable Angina) J Am Coll Cardiol. 2002;40:1366–1374. - PubMed
-
- Bertrand ME, Simoons ML, Fox KA, Wallentin LC, Hamm CW, McFadden E, de Feyter PJ, Specchia G, Ruzyllo W. Management of acute coronary syndromes: acute coronary syndromes without persistent ST-segment elevation; recommendations of the Task Force of the European Society of Cardiology. Eur Heart J. 2000;21:1406–1432. - PubMed
-
- The PRISM-PLUS Study Investigators. Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina and non-Q-wave myocardial infarction. N Engl J Med. 1998;338:1488–1497. - PubMed
-
- The PURSUIT Trial Investigators. Inhibition of platelet glycoprotein IIb/IIIa with eptifibatide in patients with acute coronary syndromes. N Engl J Med. 1998;339:436–443. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
