

Modulation of gonadotropin-releasing hormone pulse generator sensitivity to progesterone inhibition in hyperandrogenic adolescent girls--implications for regulation of pubertal maturation
- PMID: 19351732
- PMCID: PMC2708962
- DOI: 10.1210/jc.2008-2606
Modulation of gonadotropin-releasing hormone pulse generator sensitivity to progesterone inhibition in hyperandrogenic adolescent girls--implications for regulation of pubertal maturation
Abstract
Context: Adult women with polycystic ovary syndrome (PCOS) have decreased GnRH pulse generator sensitivity to progesterone (P)-mediated slowing. This defect is androgen mediated because it is reversed with androgen receptor blockade. Adolescent hyperandrogenism often precedes PCOS.
Objective: The aim of the study was to evaluate GnRH pulse generator sensitivity to P-mediated slowing in normal and hyperandrogenic girls.
Design: We conducted a controlled interventional study.
Setting: The study was conducted in a general clinical research center.
Participants: A total of 26 normal control (NC) and 26 hyperandrogenic (HA) girls were studied.
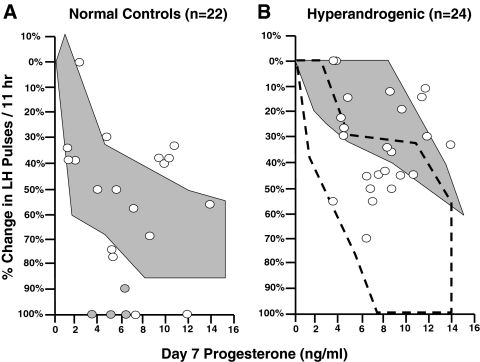
Intervention: Frequent blood sampling was performed for 11 h to assess LH pulse frequency before and after 7 d of oral estradiol and P.
Main outcome measure: We measured the slope of the percentage reduction in LH pulse frequency as a function of d 7 P (slope).
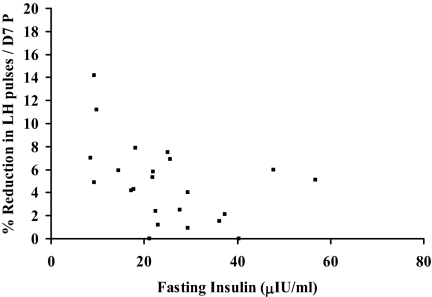
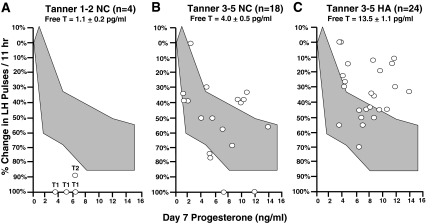
Results: Overall, Tanner 3-5 HA subjects were less sensitive to P-mediated slowing than Tanner 3-5 NC (slope, 4.7 +/- 3.4 vs. 10.3 +/- 7.7; P = 0.006). However, there was variability in the responses of HA subjects; 15 had P sensitivities within the range seen in NC, whereas nine were relatively P insensitive. The two groups had similar testosterone levels. Fasting insulin levels were higher in P-insensitive HA girls (39.6 +/- 30.6 vs. 22.2 +/- 13.9 microIU/ml; P = 0.02), and there was an inverse relationship between fasting insulin and P sensitivity in HA girls (P = 0.02). Tanner 1-2 NC had lower testosterone levels and were more P sensitive than Tanner 3-5 NC (slope, 19.3 +/- 5.8; P = 0.04).
Conclusions: Hyperandrogenism is variably associated with reduced GnRH pulse generator sensitivity to P-mediated slowing during adolescence. In addition to androgen levels, insulin resistance may modulate P sensitivity.
Figures
Comment in
-
Polycystic ovary syndrome: a model of combinatorial endocrinology?J Clin Endocrinol Metab. 2009 Jul;94(7):2250-1. doi: 10.1210/jc.2009-0959. J Clin Endocrinol Metab. 2009. PMID: 19584198 No abstract available.
References
-
- Asunción M, Calvo RM, San Millán JL, Sancho J, Avila S, Escobar-Morreale HF 2000 A prospective study of the prevalence of the polycystic ovary syndrome in unselected Caucasian women from Spain. J Clin Endocrinol Metab 85:2434–2438 - PubMed
-
- Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, Yildiz BO 2004 The prevalence and features of the polycystic ovary syndrome in an unselected population. J Clin Endocrinol Metab 89:2745–2749 - PubMed
-
- Diamanti-Kandarakis E, Kouli CR, Bergiele AT, Filandra FA, Tsianateli TC, Spina GG, Zapanti ED, Bartzis MI 1999 A survey of the polycystic ovary syndrome in the Greek island of Lesbos: hormonal and metabolic profile. J Clin Endocrinol Metab 84:4006–4011 - PubMed
-
- Zawadski J, Dunaif A 1992 Diagnostic criteria for polycystic ovary syndrome: towards a rational approach. In: Dunaif A, Givens J, Haseltine F, Merriam G, eds. Polycystic ovary syndrome. Oxford, UK: Blackwell Scientific; 377–384
-
- Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF, Futterweit W, Janssen OE, Legro RS, Norman RJ, Taylor AE, Witchel SF 2006 Position statement: criteria for defining polycystic ovary syndrome as a predominantly hyperandrogenic syndrome: an Androgen Excess Society guideline. J Clin Endocrinol Metab 91:4237–4245 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- T32 HD07383/HD/NICHD NIH HHS/United States
- K23 HD044742/HD/NICHD NIH HHS/United States
- U54 HD28934/HD/NICHD NIH HHS/United States
- U54-HD34179/HD/NICHD NIH HHS/United States
- T32 HD007383/HD/NICHD NIH HHS/United States
- F32 HD055014/HD/NICHD NIH HHS/United States
- U54 HD012303/HD/NICHD NIH HHS/United States
- U54-HD12303/HD/NICHD NIH HHS/United States
- M01 RR00827/RR/NCRR NIH HHS/United States
- U54 HD028934/HD/NICHD NIH HHS/United States
- P50 HD012303/HD/NICHD NIH HHS/United States
- M01 RR00847/RR/NCRR NIH HHS/United States
- M01 RR000827/RR/NCRR NIH HHS/United States
- M01 RR000847/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
