

A bench study of intensive-care-unit ventilators: new versus old and turbine-based versus compressed gas-based ventilators
- PMID: 19352622
- PMCID: PMC2873304
- DOI: 10.1007/s00134-009-1467-7
A bench study of intensive-care-unit ventilators: new versus old and turbine-based versus compressed gas-based ventilators
Abstract
Objective: To compare 13 commercially available, new-generation, intensive-care-unit (ICU) ventilators in terms of trigger function, pressurization capacity during pressure-support ventilation (PSV), accuracy of pressure measurements, and expiratory resistance.
Design and setting: Bench study at a research laboratory in a university hospital.
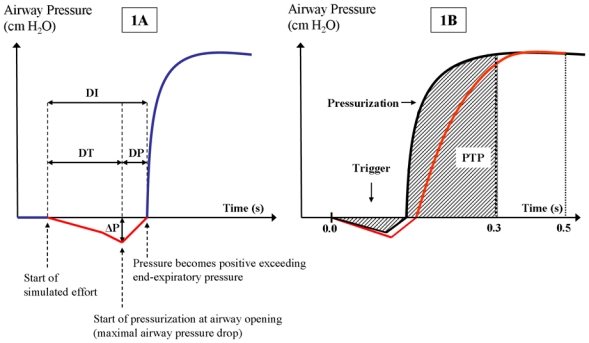
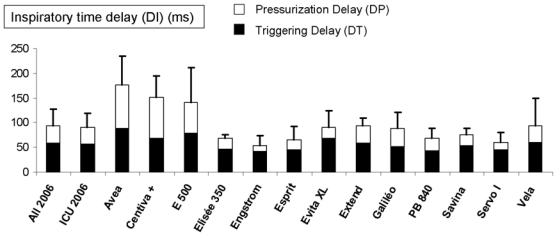
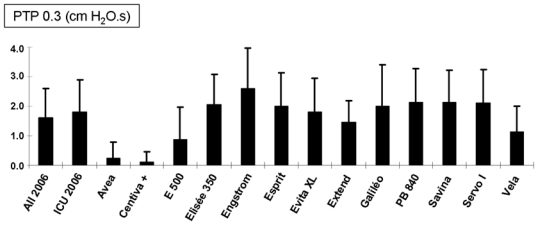
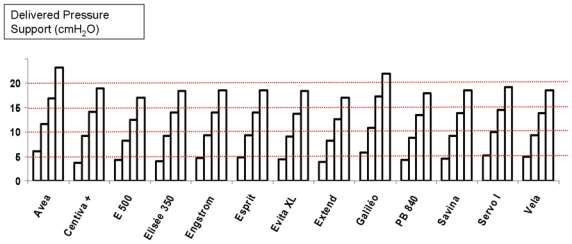
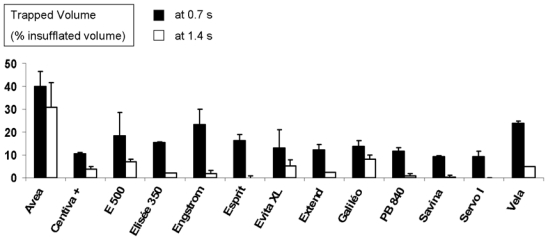
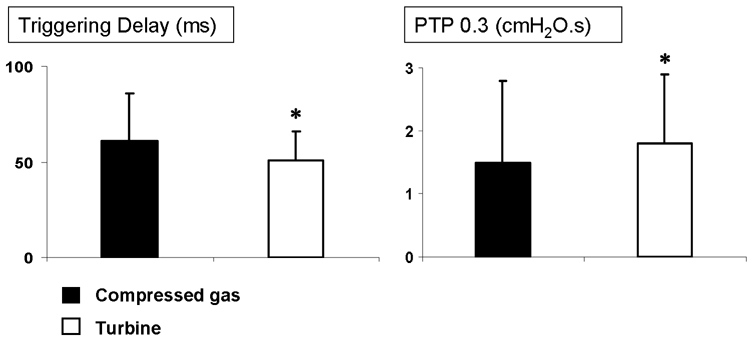
Methods: Four turbine-based ventilators and nine conventional servo-valve compressed-gas ventilators were tested using a two-compartment lung model. Three levels of effort were simulated. Each ventilator was evaluated at four PSV levels (5, 10, 15, and 20 cm H2O), with and without positive end-expiratory pressure (5 cm H2O). Trigger function was assessed as the time from effort onset to detectable pressurization. Pressurization capacity was evaluated using the airway pressure-time product computed as the net area under the pressure-time curve over the first 0.3 s after inspiratory effort onset. Expiratory resistance was evaluated by measuring trapped volume in controlled ventilation.
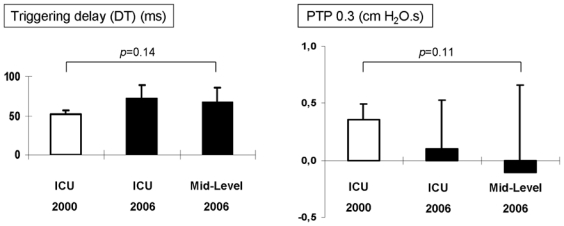
Results: Significant differences were found across the ventilators, with a range of triggering delays from 42 to 88 ms for all conditions averaged (P < 0.001). Under difficult conditions, the triggering delay was longer than 100 ms and the pressurization was poor for five ventilators at PSV5 and three at PSV10, suggesting an inability to unload patient's effort. On average, turbine-based ventilators performed better than conventional ventilators, which showed no improvement compared to a bench comparison in 2000.
Conclusion: Technical performance of trigger function, pressurization capacity, and expiratory resistance differs considerably across new-generation ICU ventilators. ICU ventilators seem to have reached a technical ceiling in recent years, and some ventilators still perform inadequately.
Figures
References
-
- Tobin MJ, Jubran A, Laghi F. Patient-ventilator interaction. Am J Respir Crit Care Med. 2001;163:1059–1063. - PubMed
-
- Esteban A, Ferguson ND, Meade MO, Frutos-Vivar F, Apezteguia C, Brochard L, Raymondos K, Nin N, Hurtado J, Tomicic V, Gonzalez M, Elizalde J, Nightingale P, Abroug F, Pelosi P, Arabi Y, Moreno R, Jibaja M, Empaire DG, Sandi F, Matamis D, Montanez AM, Anzueto A. Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med. 2008;177:170–177. - PubMed
-
- Carlucci A, Richard JC, Wysocki M, Lepage E, Brochard L. Noninvasive versus conventional mechanical ventilation. An epidemiologic survey. Am J Respir Crit Care Med. 2001;163:874–880. - PubMed
-
- Demoule A, Girou E, Richard JC, Taille S, Brochard L. Increased use of noninvasive ventilation in French intensive care units. Intensive Care Med. 2006;32:1747–1755. - PubMed
-
- Thille AW, Rodriguez P, Cabello B, Lellouche F, Brochard L. Patient-ventilator asynchrony during assisted mechanical ventilation. Intensive Care Med. 2006;32:1515–1522. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
