

Cardiac magnetic resonance assessment of dyssynchrony and myocardial scar predicts function class improvement following cardiac resynchronization therapy
- PMID: 19356481
- PMCID: PMC2678755
- DOI: 10.1016/j.jcmg.2008.04.013
Cardiac magnetic resonance assessment of dyssynchrony and myocardial scar predicts function class improvement following cardiac resynchronization therapy
Abstract
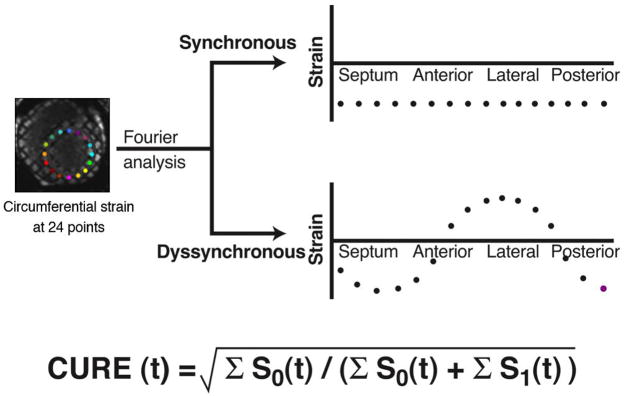
Objectives: We tested a circumferential mechanical dyssynchrony index (circumferential uniformity ratio estimate [CURE]; 0 to 1, 1 = synchrony) derived from magnetic resonance-myocardial tagging (MR-MT) for predicting clinical function class improvement following cardiac resynchronization therapy (CRT).
Background: There remains a significant nonresponse rate to CRT. MR-MT provides high quality mechanical activation data throughout the heart, and delayed enhancement cardiac magnetic resonance (DE-CMR) offers precise characterization of myocardial scar.
Methods: MR-MT was performed in 2 cohorts of heart failure patients with: 1) a CRT heart failure cohort (n = 20; left ventricular ejection fraction of 0.23 +/- 0.057) to evaluate the role of MR-MT and DE-CMR prior to CRT; and 2) a multimodality cohort (n = 27; ejection fraction of 0.20 +/- 0.066) to compare MR-MT and tissue Doppler imaging septal-lateral delay for assessment of mechanical dyssynchrony. MR-MT was also performed in 9 healthy control subjects.
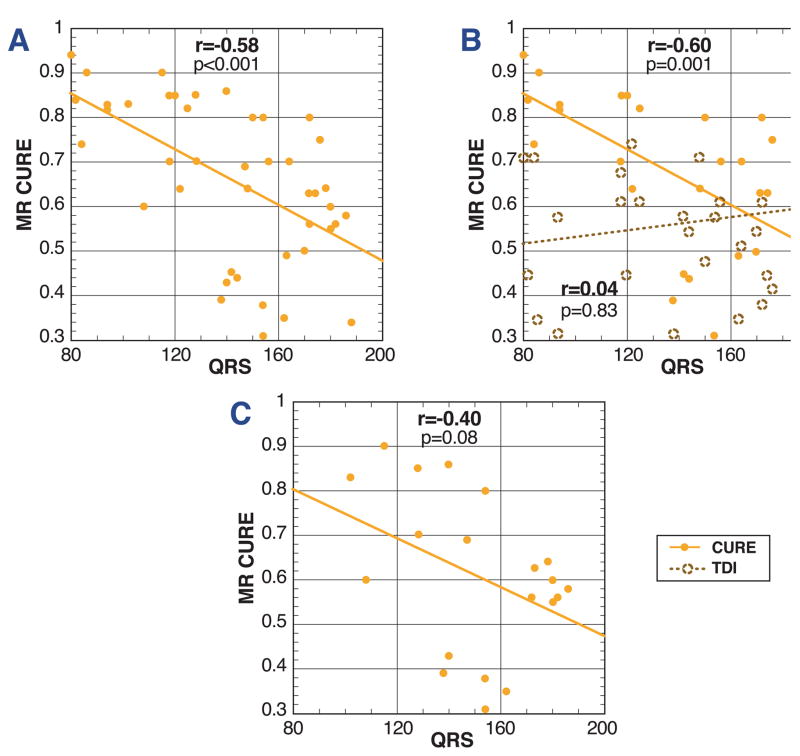
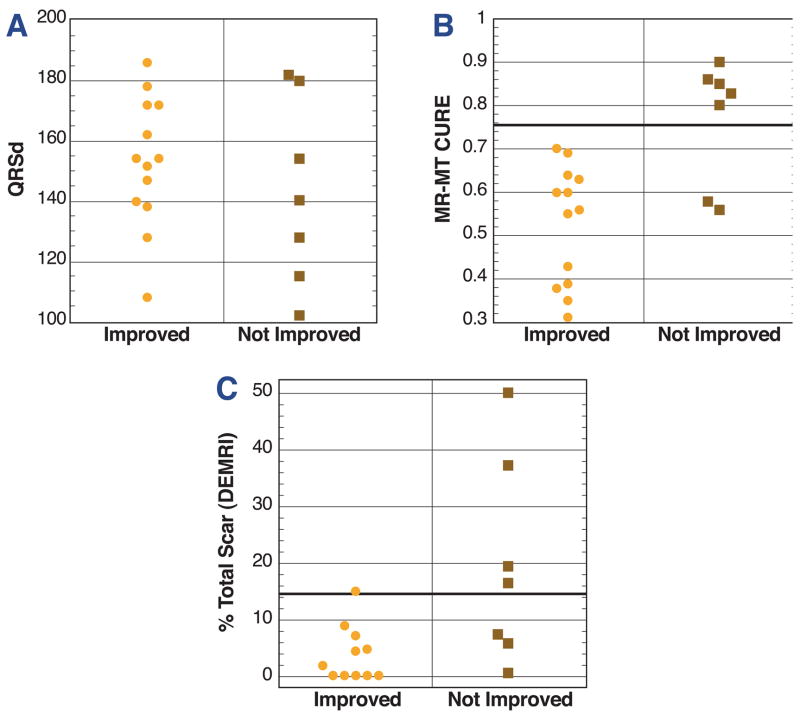
Results: MR-MT showed that control subjects had highly synchronous contraction (CURE 0.96 +/- 0.01), but tissue Doppler imaging indicated dyssynchrony in 44%. Using a cutoff of <0.75 for CURE based on receiver-operator characteristic analysis (area under the curve: 0.889), 56% of patients tested positive for mechanical dyssynchrony, and the MR-MT CURE predicted improved function class with 90% accuracy (positive and predictive values: 87%, 100%); adding DE-CMR (% total scar <15%) data improved accuracy further to 95% (positive and negative predictive values: 93%, 100%). The correlation between CURE and QRS duration was modest in all cardiomyopathy subjects (r = 0.58, p < 0.001). The multimodality cohort showed a 30% discordance rate between CURE and tissue Doppler imaging septal-lateral delay.
Conclusions: The MR-MT assessment of circumferential mechanical dyssynchrony predicts improvement in function class after CRT. The addition of scar imaging by DE-CMR further improves this predictive value.
Figures
Comment in
-
Is the magnet a better crystal ball for predicting response to cardiac resynchronization therapy?JACC Cardiovasc Imaging. 2008 Sep;1(5):569-71. doi: 10.1016/j.jcmg.2008.07.002. JACC Cardiovasc Imaging. 2008. PMID: 19356482 No abstract available.
References
-
- Bristow MR, Saxon LA, Boehmer J, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140–2150. - PubMed
-
- Cleland JG, Daubert JC, Erdmann E, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539–1549. - PubMed
-
- Chung ES, Leon AR, Tavazzi L, Nihoyannopoulos P, Merlino J, Abraham WT, Leclercq C. Predictors of Response to CRT (PROSPECT Study) Circulation. 2008 In Press. - PubMed
-
- Bleeker GB, Schalij MJ, Boersma E, et al. Relative merits of M-mode echocardiography and tissue Doppler imaging for prediction of response to cardiac resynchronization therapy in patients with heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol. 2007;99:68–74. - PubMed
-
- Lardo AC, Abraham TP, Kass DA. Magnetic resonance imaging assessment of ventricular dyssynchrony: current and emerging concepts. J Am Coll Cardiol. 2005;46:2223–2228. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
