

Three-dimensional coronary artery microscopy by intracoronary optical frequency domain imaging
- PMID: 19356512
- PMCID: PMC2852244
- DOI: 10.1016/j.jcmg.2008.06.007
Three-dimensional coronary artery microscopy by intracoronary optical frequency domain imaging
Abstract
Objectives: We present the first clinical experience with intracoronary optical frequency domain imaging (OFDI) in human patients.
Background: Intracoronary optical coherence tomography (OCT) is a catheter-based optical imaging modality that is capable of providing microscopic (approximately 7-microm axial resolution, approximately 30-microm transverse resolution), cross-sectional images of the coronary wall. Although the use of OCT has shown substantial promise for imaging coronary microstructure, blood attenuates the OCT signal, necessitating prolonged, proximal occlusion to screen long arterial segments. OFDI is a second-generation form of OCT that is capable of acquiring images at much higher frame rates. The increased speed of OFDI enables rapid, 3-dimensional imaging of long coronary segments after a brief, nonocclusive saline purge.
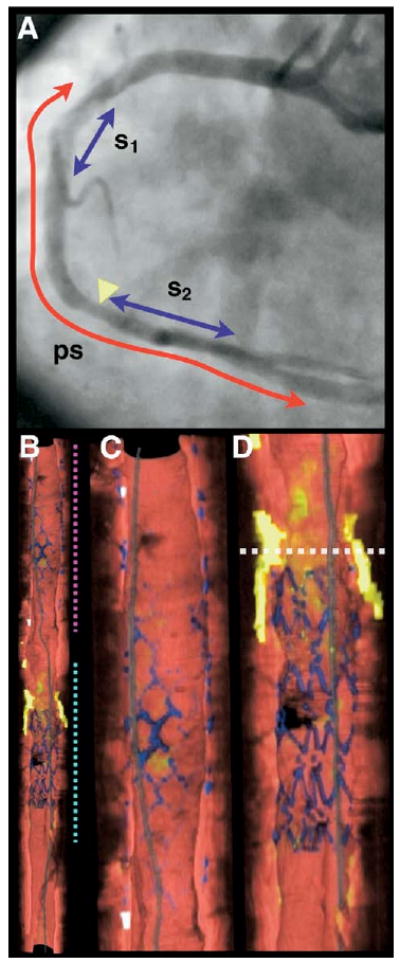
Methods: Volumetric OFDI images were obtained in 3 patients after intracoronary stent deployment. Imaging was performed in the left anterior descending and right coronary arteries with the use of a nonocclusive saline purge rates ranging from 3 to 4 ml/s and for purge durations of 3 to 4 s. After imaging, the OFDI datasets were segmented using previously documented criteria and volume rendered.
Results: Good visualization of the artery wall was obtained in all cases, with clear viewing lengths ranging from 3.0 to 7.0 cm at pullback rates ranging from 5 to 20 mm/s. A diverse range of microscopic features were identified in 2 and 3 dimensions, including thin-capped fibroatheromas, calcium, macrophages, cholesterol crystals, bare stent struts, and stents with neointimal hyperplasia. There were no complications of the OFDI procedure.
Conclusions: Our results demonstrate that OFDI is a viable method for imaging the microstructure of long coronary segments in patients. Given its ability to provide microscopic information in a practical manner, this technology may be useful for studying human coronary pathophysiology in vivo and as a clinical tool for guiding the management of coronary artery disease.
Figures






Comment in
-
Googling the coronary: fiberoptics and a computer provide the answers.JACC Cardiovasc Imaging. 2008 Nov;1(6):762-4. doi: 10.1016/j.jcmg.2008.07.015. JACC Cardiovasc Imaging. 2008. PMID: 19356513 No abstract available.
-
3D reconstructions of optical frequency domain imaging to improve understanding of conventional PCI.JACC Cardiovasc Imaging. 2011 Sep;4(9):1044-6. doi: 10.1016/j.jcmg.2011.04.018. JACC Cardiovasc Imaging. 2011. PMID: 21920344 No abstract available.
References
-
- Brezinski ME, Tearney GJ, Bouma BE, et al. Imaging of coronary artery microstructure (in vitro) with optical coherence tomography. Am J Cardiol. 1996;77:92–3. - PubMed
-
- Tearney GJ, Brezinski ME, Boppart SA, et al. Images in cardiovascular medicine. Catheter-based optical imaging of a human coronary artery Circulation. 1996;94:3013. - PubMed
-
- Tearney GJ, Jang IK, Kang DH, et al. Porcine coronary imaging in vivo by optical coherence tomography. Acta Cardiol. 2000;55:233–7. - PubMed
-
- Jang IK, Tearney G, Bouma B. Visualization of tissue prolapse between coronary stent struts by optical coherence tomography: comparison with intravascular ultrasound. Circulation. 2001;104:2754. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
