

Development of an echocardiographic risk-stratification index to predict heart failure in patients with stable coronary artery disease: the Heart and Soul study
- PMID: 19356527
- PMCID: PMC2762421
- DOI: 10.1016/j.jcmg.2008.08.004
Development of an echocardiographic risk-stratification index to predict heart failure in patients with stable coronary artery disease: the Heart and Soul study
Abstract
Objectives: We sought to determine which transthoracic echocardiographic (TTE) measurements most strongly predict heart failure (HF) and to develop an index for risk stratification in outpatients with coronary artery disease (CAD).
Background: Many TTE measurements have been shown to be predictive of HF, and they might be useful if aggregated into a risk-prediction index.
Methods: We performed TTE in 1,024 outpatients with stable CAD enrolled in the Heart and Soul study and followed them for 4.4 years. With Cox proportional hazard models, we evaluated the association of 15 TTE measurements with subsequent HF hospital stay. Those measurements that independently predicted HF were combined into an index. Variables were defined as normal or abnormal on the basis of dichotomous cutoffs determined from the American Society of Echocardiography. Abnormal variables in each measurement were assigned points on the basis of strength of association with HF.
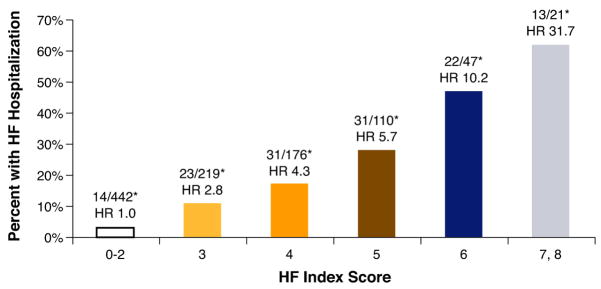
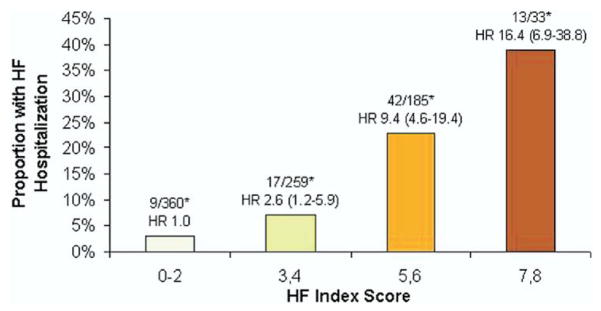
Results: Of the 15 variables, 5 measurements were independent predictors of HF: left ventricular mass index (LVMI), left atrial volume index (LAVI), mitral regurgitation (MR), left ventricular outflow tract velocity-time integral (VTI(LVOT)), and diastolic dysfunction (DD). In multivariate analysis, each of the 5 measurements independently predicted HF: LVMI >90 g/m(2) (hazard ratio [HR]: 4.1; 95% confidence interval [CI]: 2.3 to 7.2, p < 0.0001); pseudo-normal or restrictive DD (HR: 2.9; 95% CI: 1.8 to 4.5, p < 0.0001); VTI(LVOT) <22 mm (HR: 2.2; 95% CI: 1.4 to 3.5, p = 0.0004); mild, moderate, or severe MR (HR: 1.8; 95% CI: 1.2 to 2.8, p = 0.009); and LAVI >29 ml/m(2) (HR: 1.6; 95% CI: 1.0 to 2.5, p < 0.06). Combining these measurements, the Heart Failure Index ranged from 0 to 8, representing risk as follows: 3 points for LVMI, 2 points for DD, and 1 point for VTI(LVOT), MR, and LAVI. Among participants with 0 to 2 points: 4% had HF hospital stays (reference); 3 to 4 points: 10% (HR: 2.4; 95% CI: 1.3 to 4.4, p = 0.003); 5 to 6 points: 24% (HR: 6.2; 95% CI: 3.6 to 10.6, p < 0.0001); 7 to 8 points: 48% (HR: 13.7; 95% CI: 7.2 to 25.9, p < 0.0001).
Conclusions: We identified 5 TTE measurements that independently predict HF in patients with stable CAD and combined them as an index that might be useful for risk stratification and serial observations.
Figures
Comment in
-
Role of echocardiography in predicting onset of heart failure in patients with stable coronary artery disease: is the whole greater than the sum of its parts?JACC Cardiovasc Imaging. 2009 Jan;2(1):21-3. doi: 10.1016/j.jcmg.2008.10.005. JACC Cardiovasc Imaging. 2009. PMID: 19356528 No abstract available.
-
The use of echocardiography in predicting heart failure in patients with coronary artery disease.Curr Cardiol Rep. 2009 May;11(3):155-6. doi: 10.1007/s11886-009-0023-y. Curr Cardiol Rep. 2009. PMID: 19379634 No abstract available.
References
-
- Cheitlin MD, Alpert JS, Armstrong WF, et al. ACC/AHA guidelines for the clinical application of echocardiography. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Clinical Application of Echocardiography). Developed in collaboration with the American Society of Echocardiography. J Am Coll Cardiol. 1997;29:862–79. - PubMed
-
- Sundstrom J, Lind L, Arnlov J, Zethelius B, Andren B, Lithell HO. Echocardiographic and electrocardiographic diagnoses of left ventricular hypertrophy predict mortality independently of each other in a population of elderly men. Circulation. 2001;103:2346–51. - PubMed
-
- Moller JE, Hillis GS, Oh JK, et al. Left atrial volume: a powerful predictor of survival after acute myocardial infarction. Circulation. 2003;107:2207–12. - PubMed
-
- Beinart R, Boyko V, Schwammenthal E, et al. Long-term prognostic significance of left atrial volume in acute myocardial infarction. J Am Coll Cardiol. 2004;44:327–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
