

Combining GFR and albuminuria to classify CKD improves prediction of ESRD
- PMID: 19357254
- PMCID: PMC2678033
- DOI: 10.1681/ASN.2008070730
Combining GFR and albuminuria to classify CKD improves prediction of ESRD
Abstract
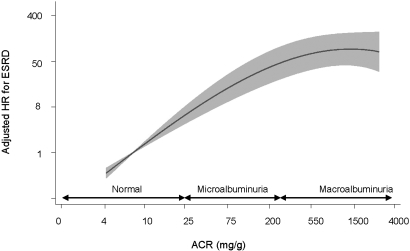
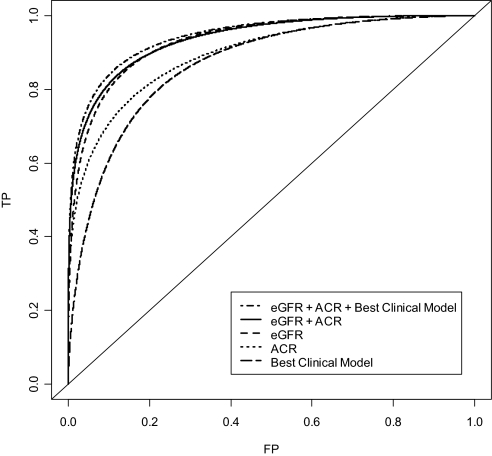
Despite the high prevalence of chronic kidney disease (CKD), relatively few individuals with CKD progress to ESRD. A better understanding of the risk factors for progression could improve the classification system of CKD and strategies for screening. We analyzed data from 65,589 adults who participated in the Nord-Trøndelag Health (HUNT 2) Study (1995 to 1997) and found 124 patients who progressed to ESRD after 10.3 yr of follow-up. In multivariable survival analysis, estimated GFR (eGFR) and albuminuria were independently and strongly associated with progression to ESRD: Hazard ratios for eGFR 45 to 59, 30 to 44, and 15 to 29 ml/min per 1.73 m(2) were 6.7, 18.8, and 65.7, respectively (P < 0.001 for all), and for micro- and macroalbuminuria were 13.0 and 47.2 (P < 0.001 for both). Hypertension, diabetes, male gender, smoking, depression, obesity, cardiovascular disease, dyslipidemia, physical activity and education did not add predictive information. Time-dependent receiver operating characteristic analyses showed that considering both the urinary albumin/creatinine ratio and eGFR substantially improved diagnostic accuracy. Referral based on current stages 3 to 4 CKD (eGFR 15 to 59 ml/min per 1.73 m(2)) would include 4.7% of the general population and identify 69.4% of all individuals progressing to ESRD. Referral based on our classification system would include 1.4% of the general population without losing predictive power (i.e., it would detect 65.6% of all individuals progressing to ESRD). In conclusion, all levels of reduced eGFR should be complemented by quantification of urinary albumin to predict optimally progression to ESRD.
Figures
Comment in
-
CKD classification: time to move beyond KDOQI.J Am Soc Nephrol. 2009 May;20(5):929-30. doi: 10.1681/ASN.2009030309. Epub 2009 Apr 23. J Am Soc Nephrol. 2009. PMID: 19389841 No abstract available.
References
-
- K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Kidney Disease Outcome Quality Initiative. Am J Kidney Dis 39: S1–S246, 2002 - PubMed
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS: Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047, 2007 - PubMed
-
- Hallan SI, Coresh J, Astor BC, Asberg A, Powe NR, Romundstad S, Hallan HA, Lydersen S, Holmen J: International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J Am Soc Nephrol 17: 2275–2284, 2006 - PubMed
-
- Crowe E, Halpin D, Stevens P, Guideline Development Group. Early identification and management of chronic kidney disease: summary of NICE guidance. BMJ 337: a153, 2008 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
