

Noncontiguous spinal tuberculosis: incidence and management
- PMID: 19357878
- PMCID: PMC2899513
- DOI: 10.1007/s00586-009-0966-0
Noncontiguous spinal tuberculosis: incidence and management
Abstract
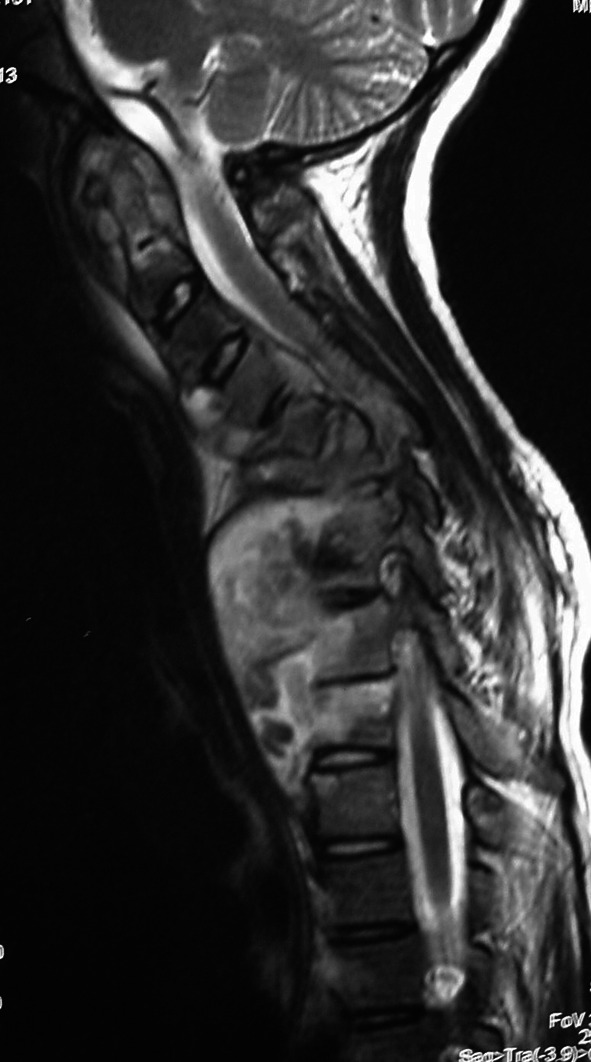
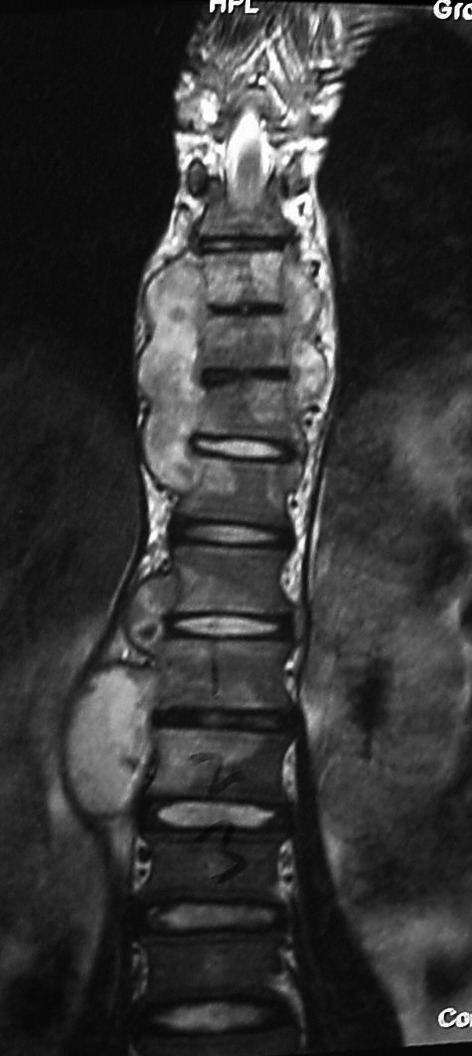
Tuberculosis (TB) has a worthy reputation as one of the great mimickers in medicine with a multitude of clinical pictures and variations. Noncontiguous spinal TB is described as atypical and case reports are published as rarities in the mainstream academic journals. The aim of the study was to asses the incidence and review of the management of non-contiguous spinal TB. We identified 16 cases of noncontiguous spinal TB from a single surgeon series of 98 patients, who were managed surgically between 2001 and 2006. These were diagnosed on whole spine MRI. This represents the largest series reported in literature to date and is higher than the expected incidence. Case notes and imaging were retrospectively reviewed in an attempt to ascertain if there were any parameters to differentiate this group from the rest of the TB spine population. Our incidence of noncontiguous spinal TB is 16.3%. There was a higher incidence of neurology in the noncontiguous group (75%) compared to the rest of our group (58.5%). Non-contiguous TB was not found to be a manifestation of HIV, MDR TB or of chronicity in our series. Most noncontiguous lesions were evident on plain radiology. Noncontiguous spinal TB is common in areas of high prevalence such as South Africa. Despite being frequently missed initially, noncontiguous involvement is evident on plain radiography and simply requires a higher index of suspicion. When investigating spine TB patients, simple radiology of the entire spine is mandatory. If available, a full spine sagittal MRI is extremely useful in identifying noncontiguous lesions. Treatment of noncontiguous tuberculosis is as for standard spinal TB cases in our unit with similar outcomes, but care needs to be taken in surgical planning as patients may have multiple areas of neurological compromise.
Figures



References
-
- Ahmadi J, Bajaj A, Destian S, Segall HD, Chi-Shing Z. Spinal tuberculosis: atypical observations at MR imaging. Radiology. 1993;189(2):489–493. - PubMed
-
- Amogne W, Abubaker A. Multifocal vertebral tuberculosis with involvement of the ribs: a case report. Ethiop Med J. 2002;40(4):397–405. - PubMed
-
- Babhulkar SS, Tayade WB, Babhulkar SK. Atypical spinal tuberculosis. J Bone Joint Surg Br. 1984;66-B(2):239–242. - PubMed
-
- Bailey HL, Gabriel M, Hodgson AR, Shin JS. Tuberculosis of the spine in children. J Bone Joint Surg Am. 1972;54:1633–1657. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
