

Computed tomography and magnetic resonance imaging appearance of renal neoplasms after radiofrequency ablation and cryoablation
- PMID: 19358438
- PMCID: PMC3047393
- DOI: 10.1053/j.sult.2008.12.005
Computed tomography and magnetic resonance imaging appearance of renal neoplasms after radiofrequency ablation and cryoablation
Abstract
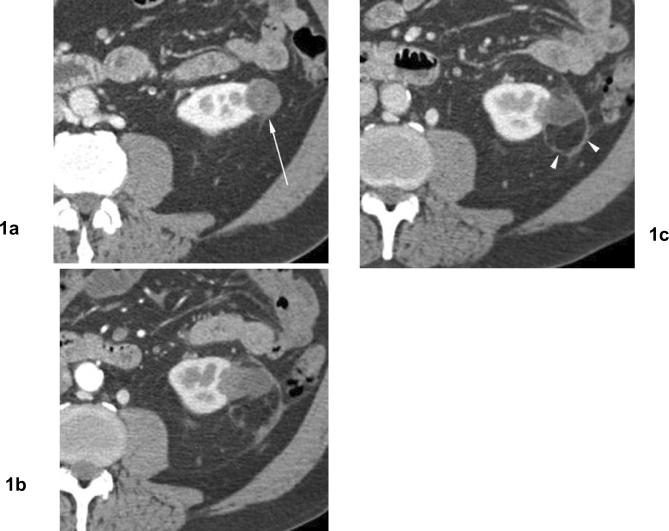
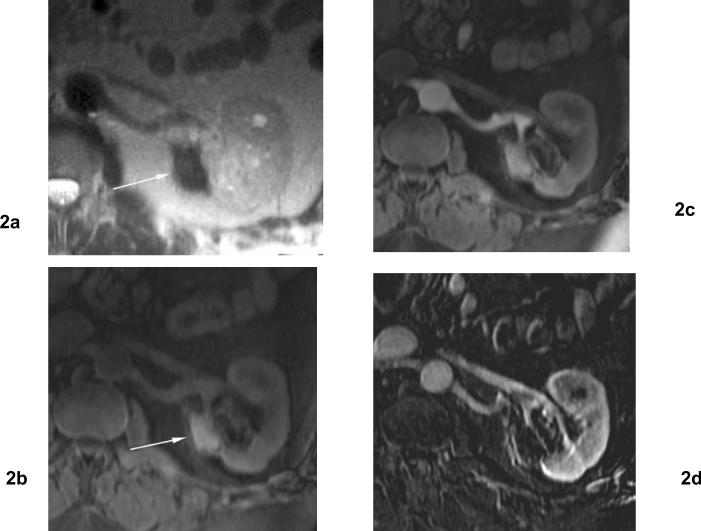
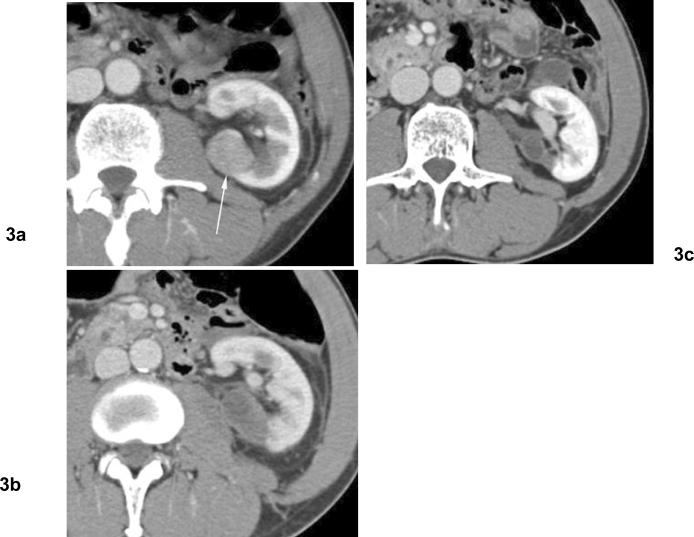
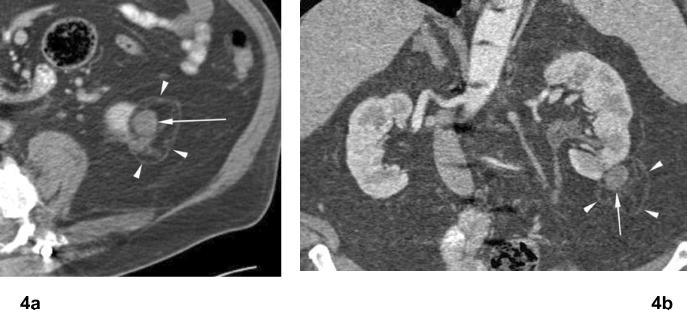
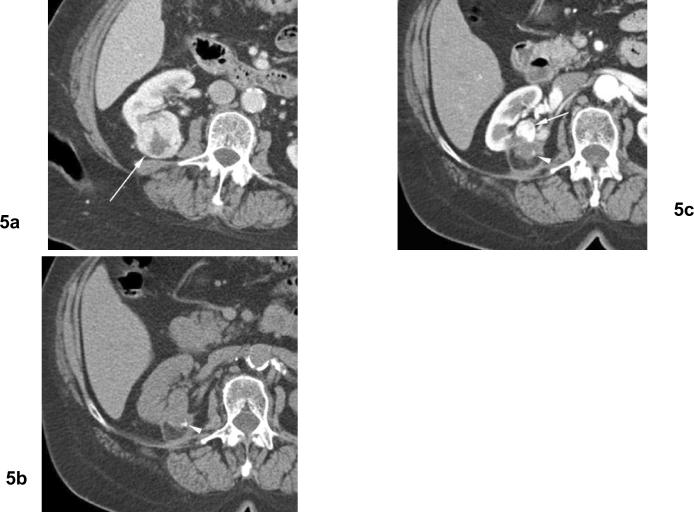
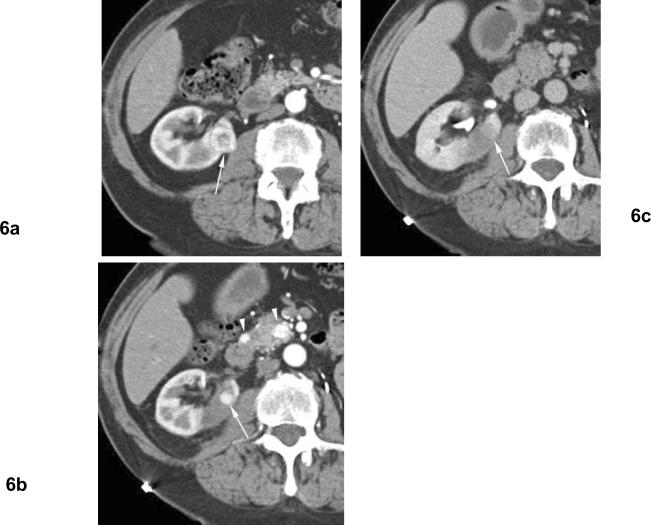
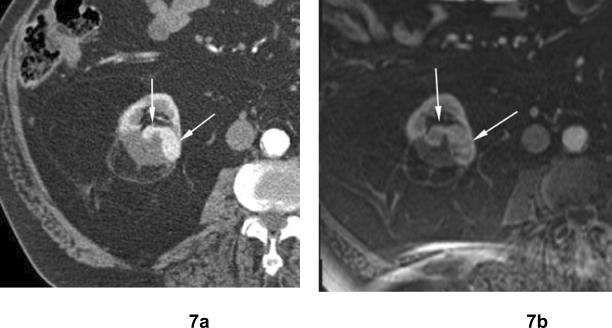
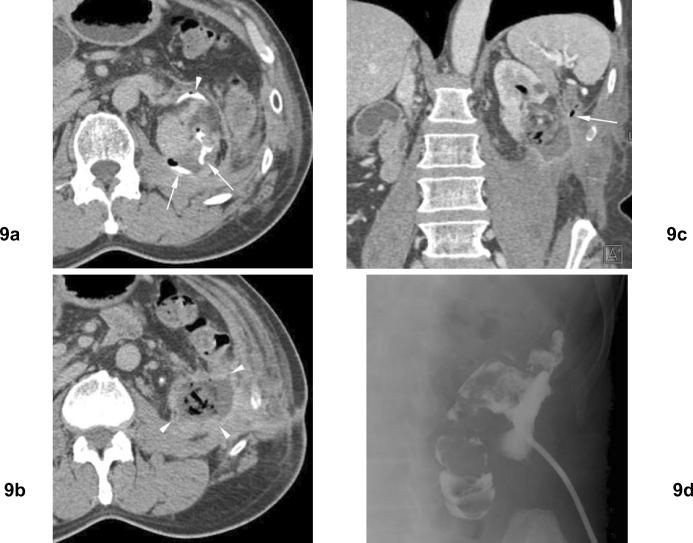
Thermal ablation procedures including radiofrequency ablation and cryoablation have been increasingly used for treatment for small renal cell carcinoma. Currently, computed tomography and magnetic resonance imaging are usually used to assess residual or recurrent disease after thermal ablation of renal tumor. After thermal ablation, the zone of ablation is usually seen as an area of hypoattenuation on computed tomography and is generally hypointense at T2-weighted magnetic resonance imaging and iso- to hyperintense at T1-weighted imaging relative to renal parenchyma. The ablation zone frequently involutes over time. Residual tumor after thermal ablation is most common at the margin of the ablation zone and often seen as nodular or crescent-shaped areas of contrast enhancement. Accurate assessment of ablated tumors at postprocedural imaging is essential for evaluating the adequacy of treatment and guiding further management. Complications are uncommon and usually minor but should be detected on postprocedural imaging studies.
Figures


References
-
- Pantuck AJ, Zisman A, Belldegrun AS. The changing natural history of renal cell carcinoma. J Urol. 2001;166(5):1611–1623. - PubMed
-
- Chow WH, Devesa SS, Warren JL, Fraumeni JF., Jr. Rising incidence of renal cell cancer in the United States. Jama. 1999;281(17):1628–1631. - PubMed
-
- Jayson M, Sanders H. Increased incidence of serendipitously discovered renal cell carcinoma. Urology. 1998;51(2):203–205. - PubMed
-
- Luciani LG, Cestari R, Tallarigo C. Incidental renal cell carcinoma-age and stage characterization and clinical implications: study of 1092 patients (1982–1997) Urology. 2000;56(1):58–62. - PubMed
-
- Fergany AF, Hafez KS, Novick AC. Long-term results of nephron sparing surgery for localized renal cell carcinoma: 10-year followup. J Urol. 2000;163(2):442–445. - PubMed
