

Detection of Taenia solium antigens and anti-T. solium antibodies in paired serum and cerebrospinal fluid samples from patients with intraparenchymal or extraparenchymal neurocysticercosis
- PMID: 19358669
- PMCID: PMC4059603
- DOI: 10.1086/597757
Detection of Taenia solium antigens and anti-T. solium antibodies in paired serum and cerebrospinal fluid samples from patients with intraparenchymal or extraparenchymal neurocysticercosis
Abstract
Background: Neurocysticercosis (NCC) is a frequent cause of epilepsy worldwide. Compared with the more common parenchymal brain cysts, extraparenchymal infections are difficult to manage and have a poor prognosis. Serological assays are used to detect circulating Taenia solium antigens or anti-T. solium antibodies in serum or cerebrospinal fluid (CSF) samples. There are no guidelines on whether to use serum or CSF specimens for a particular assay.
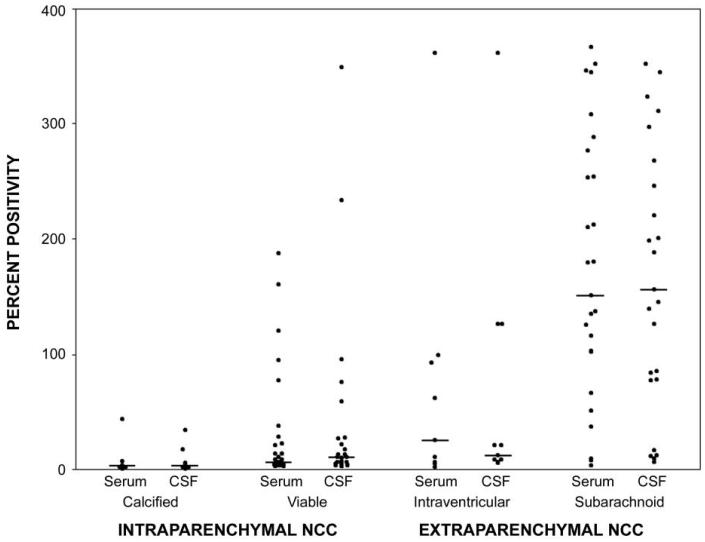
Methods: We obtained paired serum and CSF samples from 91 patients with NCC (48 had intraparenchymal NCC, and 43 had extraparenchymal NCC) for detection of antibodies, using an enzyme-linked immunotransfer blot (EITB) assay, and antigens, using a monoclonal antibody-based enzyme-linked immunosorbent assay (ELISA).
Results: For the intraparenchymal NCC group, the EITB assay yielded more true-positive results for serum samples, and the ELISA yielded slightly more true-positive results for CSF samples than for serum samples, but none of these differences were statistically significant. Most patients with calcified NCC were antibody positive but antigen negative. For extraparenchymal disease, all samples were antibody positive, and all but 2 were antigen positive, with most samples containing high antigen levels.
Conclusions: The sensitivity of antibody-detecting EITB assays is not increased through the use of CSF samples rather than serum samples. The antigen-detecting ELISA performed better for CSF samples than for serum samples, but for both specimen types it was less sensitive than the EITB assay. Active and inactive NCC are better differentiated from each other by the antigen-detecting ELISA, for both serum and CSF samples. High antigen levels suggest the presence of subarachnoid NCC.
Figures
Comment in
-
New developments in the management of neurocysticercosis.J Infect Dis. 2009 May 1;199(9):1261-2. doi: 10.1086/597758. J Infect Dis. 2009. PMID: 19358667 No abstract available.
References
-
- White AC., Jr. Neurocysticercosis: a major cause of neurological disease worldwide. Clin Infect Dis. 1997;24:101–13. - PubMed
-
- Del Brutto OH, Sotelo J. Neurocysticercosis: an update. Rev Infect Dis. 1988;10:1075–87. - PubMed
-
- Commission on Tropical Diseases of the International League against Epilepsy Relationship between epilepsy and tropical diseases. Epilepsia. 1994;35:89–93. - PubMed
-
- Mervis B, Lotz JW. Computed tomography (CT) in parenchymatous cerebral cysticercosis. Clin Radiol. 1980;31:521–8. - PubMed
