

Prospective analysis of neuropsychiatric events in an international disease inception cohort of patients with systemic lupus erythematosus
- PMID: 19359262
- PMCID: PMC2929162
- DOI: 10.1136/ard.2008.106351
Prospective analysis of neuropsychiatric events in an international disease inception cohort of patients with systemic lupus erythematosus
Abstract
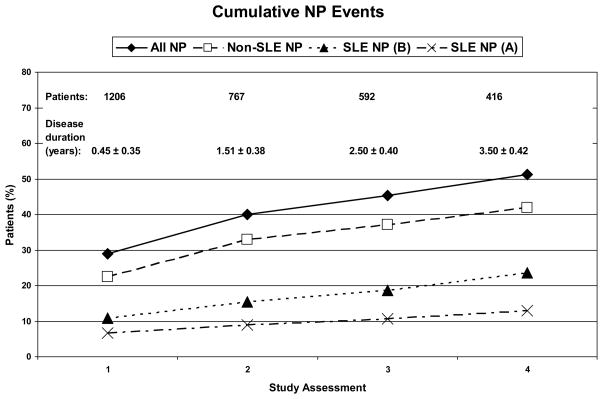
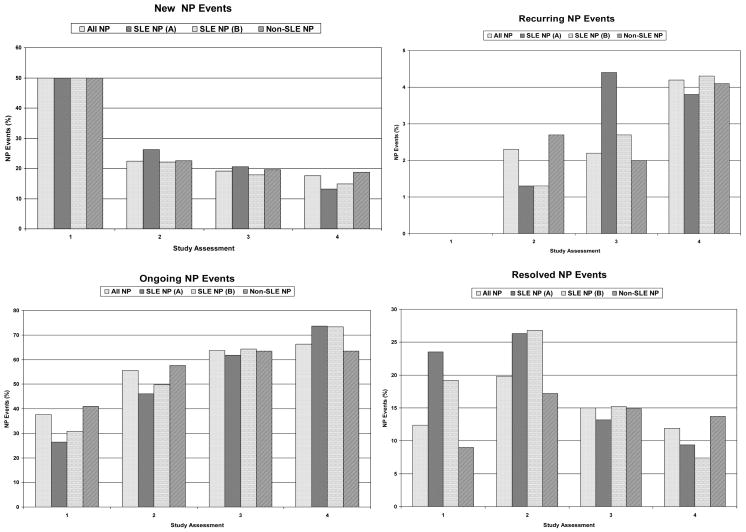
Objectives: To determine the frequency, accrual, attribution and outcome of neuropsychiatric (NP) events and impact on quality of life over 3 years in a large inception cohort of patients with systemic lupus erythematosus (SLE).
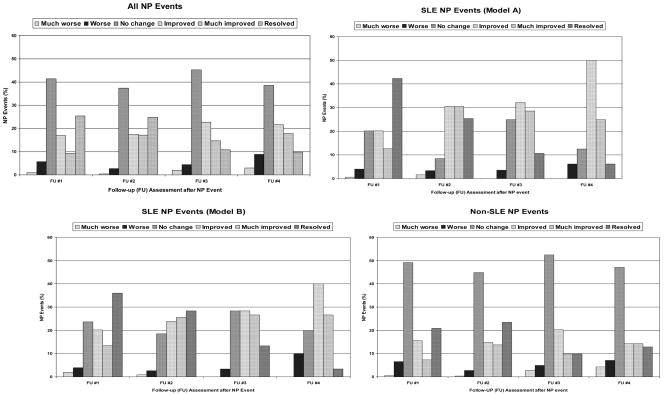
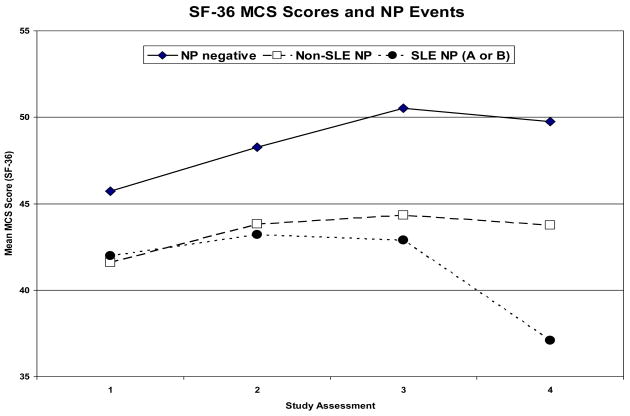
Methods: The study was conducted by the Systemic Lupus International Collaborating Clinics. Patients were enrolled within 15 months of SLE diagnosis. NP events were identified using the American College of Rheumatology case definitions, and decision rules were derived to determine the proportion of NP disease attributable to SLE. The outcome of NP events was recorded and patient-perceived impact determined by the SF-36.
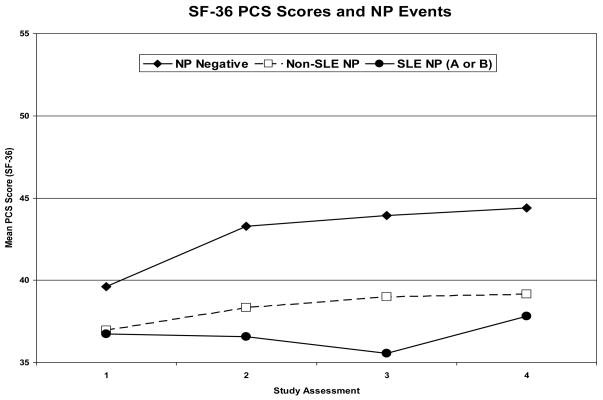
Results: 1206 patients (89.6% female) with a mean (+/-SD) age of 34.5+/-13.2 years were included in the study. The mean disease duration at enrollment was 5.4+/-4.2 months. Over a mean follow-up of 1.9+/-1.2 years, 486/1206 (40.3%) patients had > or =1 NP events, which were attributed to SLE in 13.0-23.6% of patients using two a priori decision rules. The frequency of individual NP events varied from 47.1% (headache) to 0% (myasthenia gravis). The outcome was significantly better for those NP events attributed to SLE, especially if they occurred within 1.5 years of the diagnosis of SLE. Patients with NP events, regardless of attribution, had significantly lower summary scores for both mental and physical health over the study.
Conclusions: NP events in patients with SLE are of variable frequency, most commonly present early in the disease course and adversely impact patients' quality of life over time. Events attributed to non-SLE causes are more common than those due to SLE, although the latter have a more favourable outcome.
Figures
References
-
- Ainiala H, Hietaharju A, Loukkola J, Peltola J, Korpela M, Metsanoja R, et al. Validity of the new American College of Rheumatology criteria for neuropsychiatric lupus syndromes: a population-based evaluation. Arthritis Rheum. 2001;45(5):419–23. - PubMed
-
- Brey RL, Holliday SL, Saklad AR, Navarrete MG, Hermosillo-Romo D, Stallworth CL, et al. Neuropsychiatric syndromes in lupus: prevalence using standardized definitions. Neurology. 2002;58(8):1214–20. - PubMed
-
- Hanly JG, McCurdy G, Fougere L, Douglas JA, Thompson K. Neuropsychiatric events in systemic lupus erythematosus: attribution and clinical significance. J Rheumatol. 2004;31(11):2156–62. - PubMed
-
- Sanna G, Bertolaccini ML, Cuadrado MJ, Laing H, Mathieu A, Hughes GR. Neuropsychiatric manifestations in systemic lupus erythematosus: prevalence and association with antiphospholipid antibodies. J Rheumatol. 2003;30(5):985–92. - PubMed
-
- Sibbitt WL, Jr, Brandt JR, Johnson CR, Maldonado ME, Patel SR, Ford CC, et al. The incidence and prevalence of neuropsychiatric syndromes in pediatric onset systemic lupus erythematosus. J Rheumatol. 2002;29(7):1536–42. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AR046588/AR/NIAMS NIH HHS/United States
- P60 AR048095/AR/NIAMS NIH HHS/United States
- U.1052.00.009/MRC_/Medical Research Council/United Kingdom
- M01 RR000056/RR/NCRR NIH HHS/United States
- K24 AR02318;/AR/NIAMS NIH HHS/United States
- M01 RR000048/RR/NCRR NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- MOP-49529/CAPMC/ CIHR/Canada
- MOP-57752/CAPMC/ CIHR/Canada
- P60 AR 48098/AR/NIAMS NIH HHS/United States
- MC_U105261167/MRC_/Medical Research Council/United Kingdom
- K24 AR002213/AR/NIAMS NIH HHS/United States
- MO1 RR00052/RR/NCRR NIH HHS/United States
- UL1 RR025741/RR/NCRR NIH HHS/United States
- R01 AR46588/AR/NIAMS NIH HHS/United States
- M01-RR00048/RR/NCRR NIH HHS/United States
- P60 AR048098/AR/NIAMS NIH HHS/United States
- R01 AR043727/AR/NIAMS NIH HHS/United States
- ARC_/Arthritis Research UK/United Kingdom
- K24 AR002138/AR/NIAMS NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
