

Changes in racial/ethnic disparities in the prevalence of Type 2 diabetes by obesity level among US adults
- PMID: 19360513
- PMCID: PMC2744849
- DOI: 10.1080/13557850802699155
Changes in racial/ethnic disparities in the prevalence of Type 2 diabetes by obesity level among US adults
Abstract
Objective: Ethnic minority status and obesity are two independent risk factors for Type 2 diabetes (T2D). There is no clear understanding of how they may have interacted and influenced disparities in T2D prevalence over time. This study examined the trends in racial/ethnic disparities in the prevalence of T2D by weight status among US adults.
Methods: We used nationally representative data from the National Health and Nutrition Examination Surveys I (1971-1975), II (1976-1980), and III (1988-1994), and 1999-2004 among 49,574 adults aged 20-74 years. The prevalences of diagnosed and undiagnosed T2D were estimated by race/ethnicity groups (non-Hispanic White, non-Hispanic Black, and Mexican American) and body mass index (BMI) groups (normal, 18.5-24.9; overweight, 25-29.9; obese, 30-34.9; severely obese, >or=35). We used logistic regression controlling for age, gender, and education to estimate the odds ratio of T2D across race/ethnicity and BMI groups.
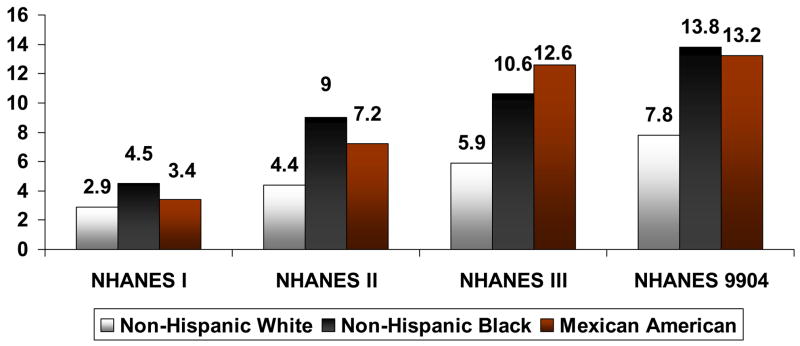
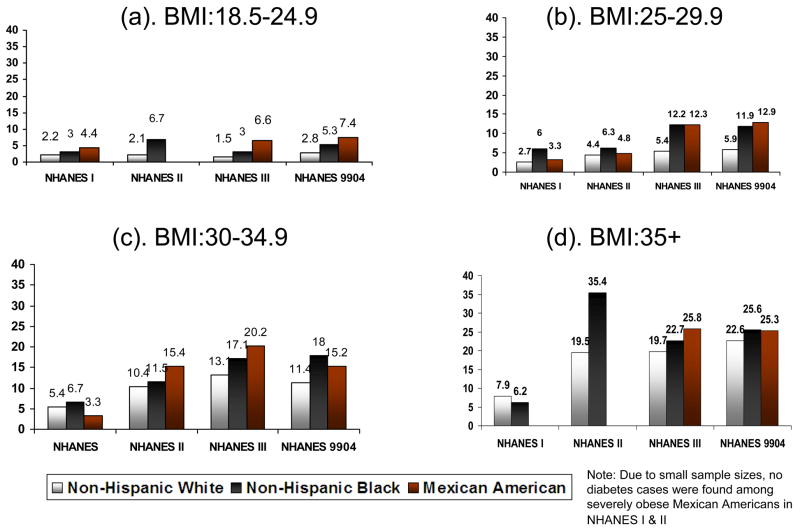
Results: Trends in racial/ethnic disparities in prevalence of diagnosed T2D varied by BMI. Normal weight group saw increasing racial disparities. In the overweight group, ethnic disparities worsened as diabetes prevalence increased 33.3% in Whites, compared to 60.0% in Blacks, and 227.3% in Mexican Americans. Minimal racial/ethnic disparities were observed in obese and severely obese groups over time. In contrast to diagnosed diabetes, overall racial/ethnic disparities in undiagnosed T2D declined in all BMI groups.
Conclusions: Racial/ethnic disparities in diabetes prevalence have become most pronounced among normal and overweight groups. Eliminating racial/ethnic disparities in diabetes will require prevention efforts not only in obese minority individuals, but also in normal and overweight minority individuals.
Figures
References
-
- Alcozer F. Secondary analysis of perceptions and meanings of type 2 diabetes among Mexican American women. The Diabetes Educator. 2000;26:785–795. - PubMed
-
- American Diabetes Association (ADA) Report of the expert committee on the diagnosis and classifcation of diabetes mellitus. Diabetes Care. 1997;20:1183–1197. - PubMed
-
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2004;27(Suppl 1):S5–s10. - PubMed
-
- Bjorntorp P. Do stress reactions cause abdominal obesity and comorbidities? Obesity Reviews. 2001;2:73–86. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical