

Post-arterial filter gaseous microemboli activity of five integral cardiotomy reservoirs during venting: an in vitro study
- PMID: 19361028
- PMCID: PMC4680219
Post-arterial filter gaseous microemboli activity of five integral cardiotomy reservoirs during venting: an in vitro study
Abstract
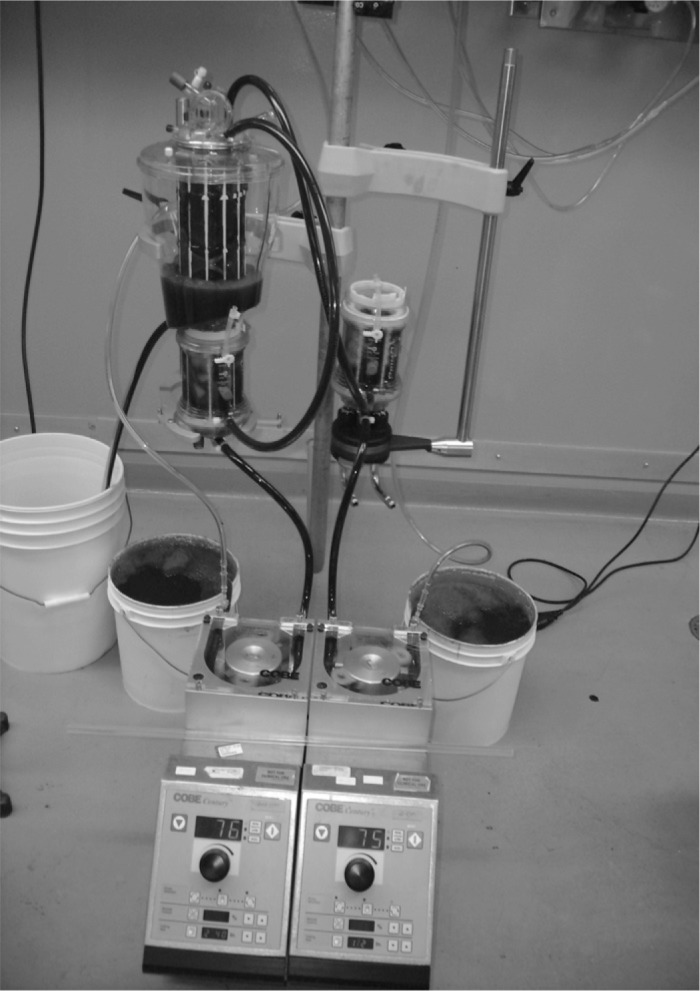
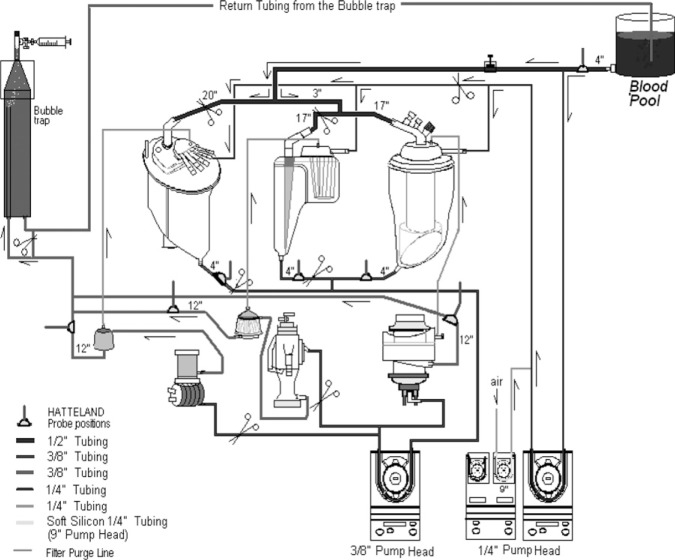
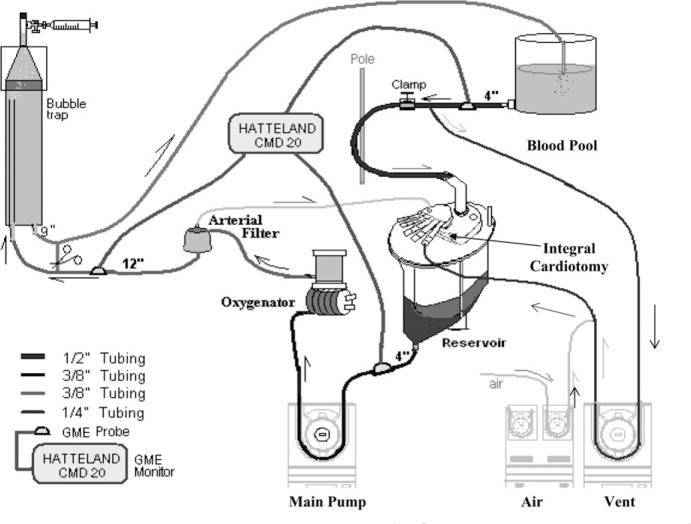
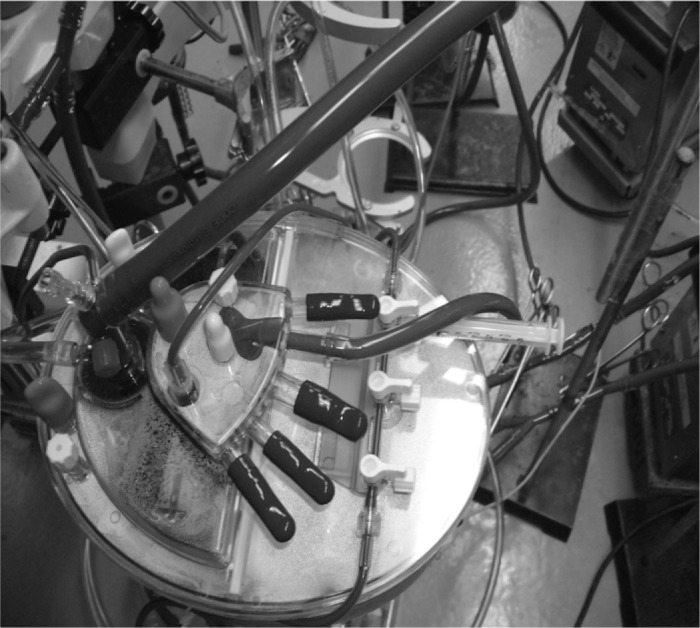
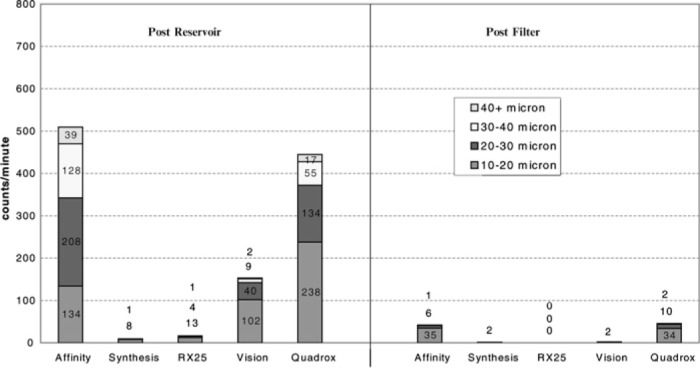
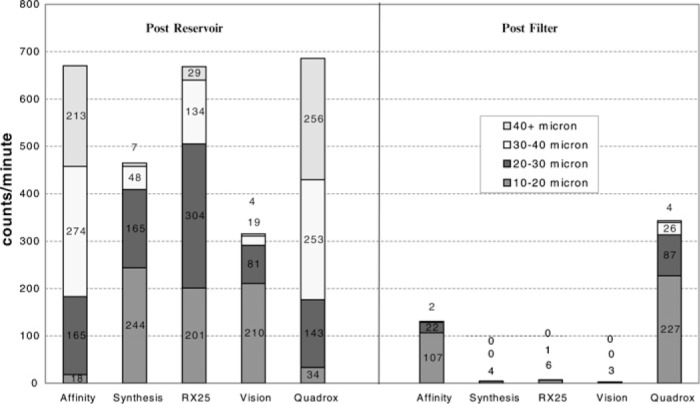
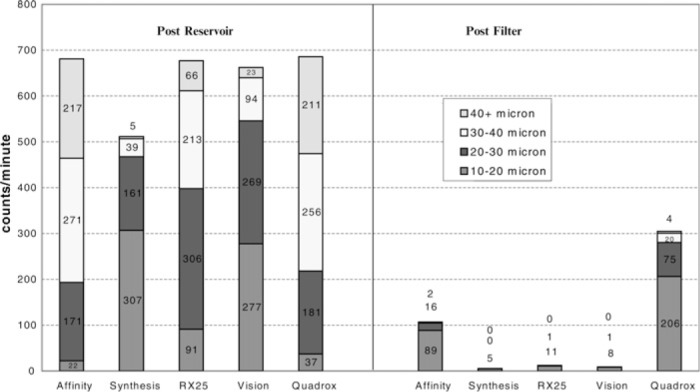
During a previously published study on gaseous microemboli (GMEs) and perfusionist interventions, it was noted that emboli could be detected after the arterial filter when blood/air challenges entered the membrane oxygenator's integral cardiotomy. The findings indicated that further study into the oxygenator's integral cardiotomy reservoir was warranted. This is the first know published report that connects the vent return to GME activity after the arterial filter. To study the air handling ability of the membranes integral cardiotomy, an in vitro study was conducted on five hard shell coated membrane oxygenators (Terumo Capiox SX25, X coated; Sorin Synthesis, phosphorylcholine coated; Gish Vision, GBS coated; Medtronic Affinity NT, trillium coated; Maquet Quadrox, bioline coated). The oxygenators were matched with their own manufacturer's coated arterial filters (Medtronic 351T Arterial Filter, Sorin Synthesis Integrated Arterial Filter, Terumo CXAF200X Arterial Filter, Gish GAF40GBS-2 Arterial Filter, and Maquet Quart HBF140 Arterial Filter). There were three arms to the study, and three separate oxygenator/filter combinations were used in each arm. The first arm consisted of a pump flow of 4.0 L/min with only the filter purge blood entering the integral cardiotomy. In the second arm, 500 mL/min of simulated vent blood was added to the filter purge blood entering the integral cardiotomy. During the final arm, 200 mL/min of air was added to the vent blood as it entered the integral cardiotomy, to more closely simulate vent return during cardiopulmonary bypass. All GME activity in the oxygenator/filter combinations was examined using the Hatteland CMD20 Microemboli Counter. Placement of the Hatteland probes was 4 in after the hard shell reservoir outlet (PRO) and 12 in after the arterial filter (PAF). When vent blood flow was turned on, there was a significant increase in the PRO microemboli activity detected in all reservoirs. In the PAF position, three of the oxygenator/filter combinations were able to remove 98-99% of the GME, one removed 84.3%, and another removed only 55.5% of the GMEs coming out of the oxygenator's reservoir. All oxygenators were found to have a dramatic increase in reservoir GME activity when the vent was turned on. Depending on the oxygenator/filter combination, vent return into the oxygenator's integral cardiotomy resulted in the presence of significant amounts of GMEs after the arterial filter.
Conflict of interest statement
This study was funded by The Sorin Group and conducted at a Sorin Group facility. Three of the co-authors are Sorin Group employees. The Synthesis oxygenator is a Sorin Group product.
Figures
References
-
- Taylor RL, Borger MA, Weisel RD, et al. . Cerebral microemboli during cardiopulmonary bypass: increased emboli during perfusionist intervention. Ann Thorac Surg. 1999;68:89–93. - PubMed
-
- Rodriguez RA, Williams KA, Babaev A, et al. . Effect of perfusionist technique on cerebral embolization during cardiopulmonary bypass. Perfusion. 2005;20:3–10. - PubMed
-
- Petrel M, Kseibi F, Sagebiel A, et al. . Comparison of conventional extracorporeal circulation (ECC) and minimal extracorporeal circulation (MECC) with regards to microbubbles and microembolic signals. Perfusion. 2005;20:329–33. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials