

The importance of myocardial amino acids during ischemia and reperfusion in dilated left ventricle of patients with degenerative mitral valve disease
- PMID: 19363596
- PMCID: PMC2850556
- DOI: 10.1007/s11010-009-0101-x
The importance of myocardial amino acids during ischemia and reperfusion in dilated left ventricle of patients with degenerative mitral valve disease
Abstract
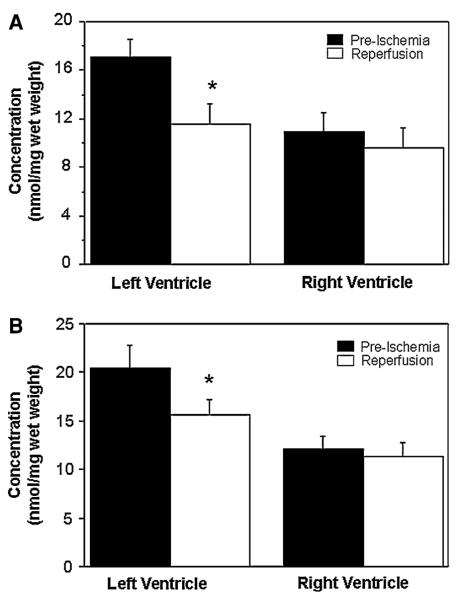
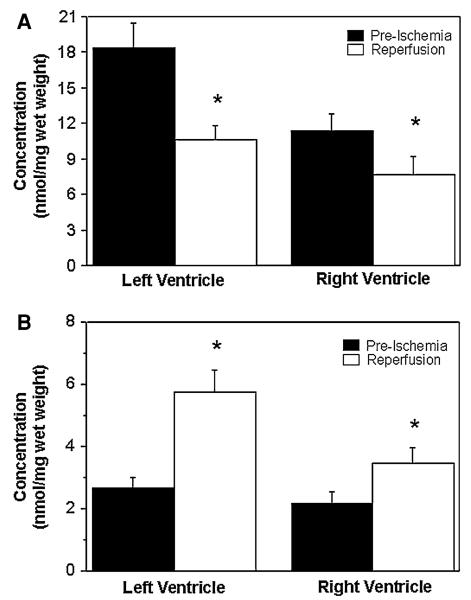
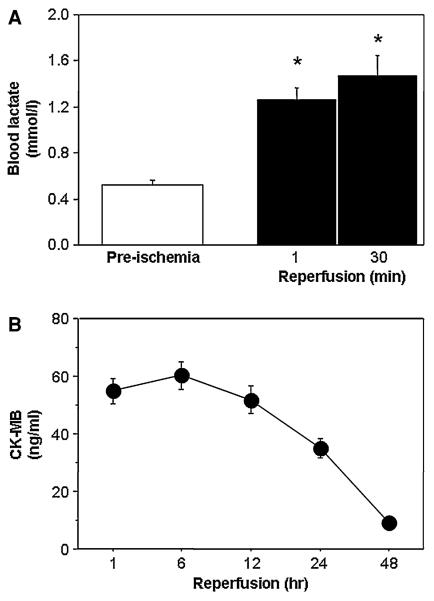
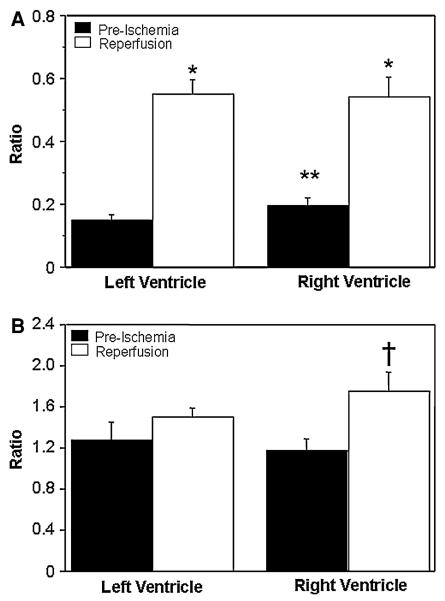
Taurine, glutamine, glutamate, aspartate, and alanine are the most abundant intracellular free amino acids in human heart. The myocardial concentration of these amino acids changes during ischemia and reperfusion due to alterations in metabolic and ionic homeostasis. We hypothesized that dilated left ventricle secondary to mitral valve disease has different levels of amino acids compared to the right ventricle and that such differences determine the extent of amino acids' changes during ischemia and reperfusion. Myocardial concentration of amino acids was measured in biopsies collected from left and right ventricles before cardioplegic arrest (Custodiol HTK) and 10 min after reperfusion in patients undergoing mitral valve surgery. The dilated left ventricle had markedly higher (P < 0.05) concentrations (nmol/mg wet weight) of taurine (17.0 +/- 1.5 vs. 10.9 +/- 1.5), glutamine (20.5 +/- 2.4 vs. 12.1 +/- 1.2), and glutamate (18.3 +/- 2.2 vs. 11.4 +/- 1.5) when compared to right ventricle. There were no differences in the basal levels of alanine or aspartate. Upon reperfusion, a significant (P < 0.05) fall in taurine and glutamine was seen only in the left ventricle. These changes are likely to be due to transport (taurine) and/or metabolism (glutamine). There was a marked increase in the alanine to glutamate ratio in both ventricles indicative of ischemic stress which was confirmed by global release of lactate during reperfusion. This study shows that in contrast to the right ventricle, the dilated left ventricle had remodeled to accumulate amino acids which are used during ischemia and reperfusion. Whether these changes reflect differences in degree of cardioplegic protection between the two ventricles remain to be investigated.
Figures
Similar articles
-
A loss of taurine and other amino acids from ventricles of patients undergoing bypass surgery.Br Heart J. 1993 Mar;69(3):241-5. doi: 10.1136/hrt.69.3.241. Br Heart J. 1993. PMID: 8461223 Free PMC article.
-
Effect of ischaemia and reperfusion on the intracellular concentration of taurine and glutamine in the hearts of patients undergoing coronary artery surgery.Biochim Biophys Acta. 1997 Mar 13;1324(2):223-31. doi: 10.1016/s0005-2736(96)00225-8. Biochim Biophys Acta. 1997. PMID: 9092709
-
Myocardial protection with intermittent cold blood during aortic valve operation: antegrade versus retrograde delivery.Ann Thorac Surg. 2003 Oct;76(4):1227-33; discussion 1233. doi: 10.1016/s0003-4975(03)00840-3. Ann Thorac Surg. 2003. PMID: 14530016 Clinical Trial.
-
Potential cardiovascular applications of glutamate, aspartate, and other amino acids.Clin Cardiol. 1998 Sep;21(9):620-4. doi: 10.1002/clc.4960210904. Clin Cardiol. 1998. PMID: 9755377 Free PMC article. Review.
-
[Refractory heart failure. Surgery of the left ventricle and mitral insufficiency].Ital Heart J Suppl. 2002 Aug;3(8):822-30. Ital Heart J Suppl. 2002. PMID: 12407837 Review. Italian.
Cited by
-
Cardiac Energy Metabolism in Heart Failure.Circ Res. 2021 May 14;128(10):1487-1513. doi: 10.1161/CIRCRESAHA.121.318241. Epub 2021 May 13. Circ Res. 2021. PMID: 33983836 Free PMC article. Review.
-
Branched-Chain Amino Acid Metabolism in the Failing Heart.Cardiovasc Drugs Ther. 2023 Apr;37(2):413-420. doi: 10.1007/s10557-022-07320-4. Epub 2022 Feb 12. Cardiovasc Drugs Ther. 2023. PMID: 35150384 Review.
-
Metabolomics assessment reveals oxidative stress and altered energy production in the heart after ischemic acute kidney injury in mice.Kidney Int. 2019 Mar;95(3):590-610. doi: 10.1016/j.kint.2018.10.020. Epub 2019 Jan 30. Kidney Int. 2019. PMID: 30709662 Free PMC article.
-
Changes in the mitochondrial function and in the efficiency of energy transfer pathways during cardiomyocyte aging.Mol Cell Biochem. 2017 Aug;432(1-2):141-158. doi: 10.1007/s11010-017-3005-1. Epub 2017 Mar 14. Mol Cell Biochem. 2017. PMID: 28293876
-
Taurine as Antioxidant in a Novel Cell- and Oxygen Carrier-Free Perfusate for Normothermic Machine Perfusion of Porcine Kidneys.Antioxidants (Basel). 2023 Mar 21;12(3):768. doi: 10.3390/antiox12030768. Antioxidants (Basel). 2023. PMID: 36979015 Free PMC article.
References
-
- Caputo M, Bryan AJ, Calafiore AM, et al. Intermittent antegrade hyperkalaemic warm blood cardioplegia supplemented with magnesium prevents myocardial substrate derangement in patients undergoing coronary artery bypass surgery. Eur J Cardiothorac Surg. 1998;14:596–601. doi:10.1016/S1010-7940(98)00247-4. - PubMed
-
- Caputo M, Dihmis WC, Bryan AJ, et al. Warm blood hyperkalaemic reperfusion (‘hot shot’) prevents myocardial substrate derangement in patients undergoing coronary artery bypass surgery. Eur J Cardiothorac Surg. 1998;13:559–564. doi:10.1016/S1010-7940(98)00056-6. - PubMed
-
- Suleiman MS, Halestrap AP, Griffiths EJ. Mitochondria: a target for myocardial protection. Pharmacol Ther. 2001;89:29–46. doi: 10.1016/S0163-7258(00)00102-9. - PubMed
-
- Tritto FP, Inserte J, Garcia-Dorado D, et al. Sodium/hydrogen exchanger inhibition reduces myocardial reperfusion edema after normothermic cardioplegia. J Thorac Cardiovasc Surg. 1998;115:709–715. doi:10.1016/S0022-5223(98)70337-X. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
