

Genomic grade index is associated with response to chemotherapy in patients with breast cancer
- PMID: 19364972
- PMCID: PMC2716940
- DOI: 10.1200/JCO.2008.18.5934
Genomic grade index is associated with response to chemotherapy in patients with breast cancer
Abstract
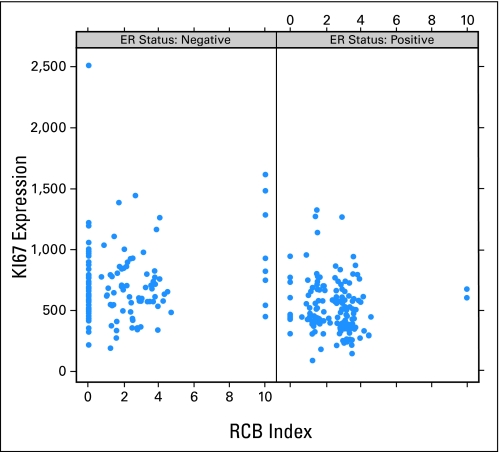
PURPOSE The genomic grade index (GGI) is a 97-gene measure of histological tumor grade. High GGI is associated with decreased relapse-free survival in patients receiving either endocrine or no systemic adjuvant therapy. Herein we examined whether GGI predicts pathologic response to neoadjuvant chemotherapy in patients with HER-2-normal breast cancer. METHODS Gene expression data (gene chips) was generated from fine-needle aspiration biopsies (n = 229) prospectively collected before neoadjuvant paclitaxel, fluorouracil, doxorubicin, and cyclophosphamide chemotherapy. Pathologic response was quantified using the residual cancer burden (RCB) method. The association between the GGI and pathologic response was assessed in univariate and multivariate analyses. The performance of a response predictor combining clinical variables and GGI was evaluated under cross-validation. Results Eighty-five percent of grade 1 tumors had low GGI, 89% of grade 3 tumors had high GGI, and 63% of grade 2 tumors had low GGI. Among both estrogen receptor (ER)-positive and -negative cancers, high GGI score was associated with pathologic complete response (RCB-0) or minimal residual disease (RCB-1). A multivariate model combining GGI and clinical parameters had an overall accuracy of 71%, compared with 58% for the GGI alone, for prediction of pathologic response. However, high GGI score was also associated with significantly worse distant relapse-free survival in patients with ER-positive cancer (P = .005), and was not associated with survival in patients with ER-negative cancer. CONCLUSION High GGI is associated with increased sensitivity to neoadjuvant paclitaxel plus fluorouracil, adriamycin, and cyclophosphamide chemotherapy in both ER-negative and ER-positive patients, but it remains a predictor of worse survival in ER-positive patients.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures





References
-
- Rakha EA, El-Sayed ME, Lee AH, et al. Prognostic significance of Nottingham histologic grade in invasive breast carcinoma. J Clin Oncol. 2008;26:3153–3158. - PubMed
-
- Trudeau ME, Pritchard KI, Chapman JA, et al. Prognostic factors affecting the natural history of node-negative breast cancer. Breast Cancer Res Trt. 2005;89:35–45. - PubMed
-
- Fisher ER, Wang J, Bryant J, et al. Pathobiology of preoperative chemotherapy: Findings from the National Surgical Adjuvant Breast and Bowel (NSABP) protocol B-18. Cancer. 2002;95:681–695. - PubMed
-
- Singletary SE, Allred C, Ashley P, et al. Revision of the American Joint Committee on Cancer staging system for breast cancer. J Clin Oncol. 2002;20:3628–3636. - PubMed
-
- Sotiriou C, Wirapati P, Loi S, et al. Gene expression profiling in breast cancer: Understanding the molecular basis of histologic grade to improve prognosis. J Natl Cancer Inst. 2006;98:262–272. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
