

Physician alerts to prevent symptomatic venous thromboembolism in hospitalized patients
- PMID: 19364975
- PMCID: PMC2901546
- DOI: 10.1161/CIRCULATIONAHA.108.841197
Physician alerts to prevent symptomatic venous thromboembolism in hospitalized patients
Erratum in
- Circulation. 2010 Jul 6;122(1):e4
Abstract
Background: Venous thromboembolism (VTE) prophylaxis remains underused among hospitalized patients. We designed and carried out a large, multicenter, randomized controlled trial to test the hypothesis that an alert from a hospital staff member to the attending physician will reduce the rate of symptomatic VTE among high-risk patients not receiving prophylaxis.
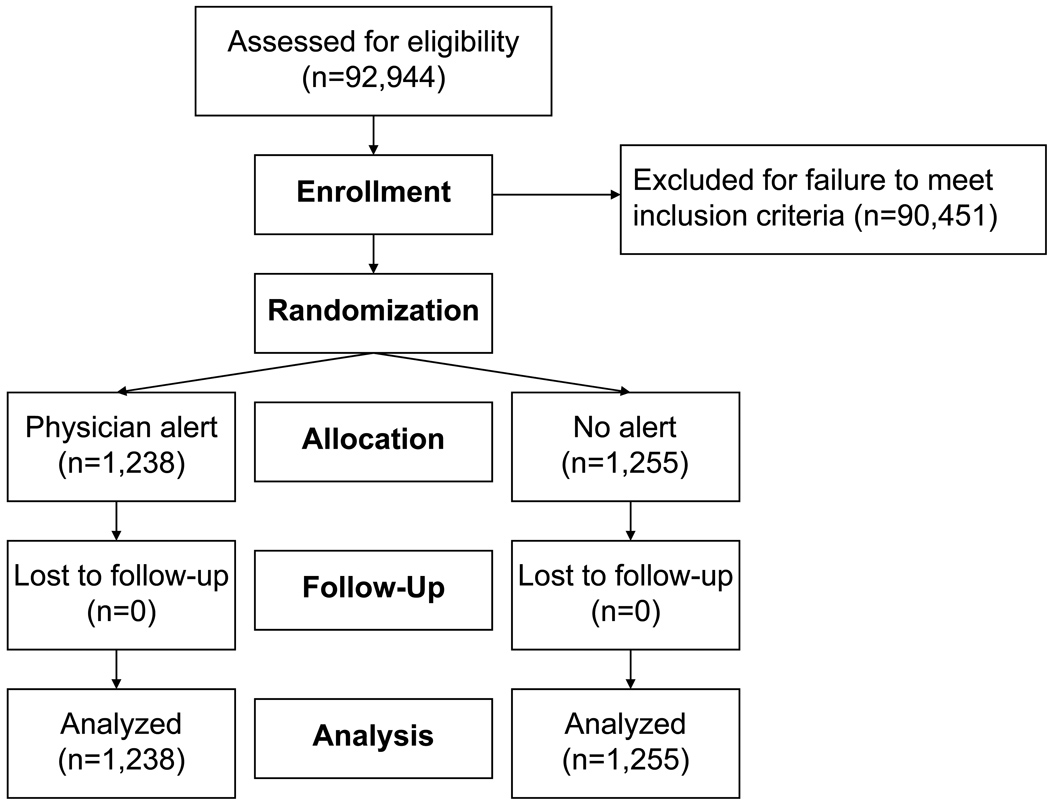
Methods and results: We enrolled patients using a validated point score system to detect hospitalized patients at high risk for symptomatic VTE who were not receiving prophylaxis. We randomized 2493 patients (82% on Medical Services) from 25 study sites to the intervention group (n=1238), in which the responsible physician was alerted by another hospital staff member, or the control group (n=1255), in which no alert was issued. The primary end point was symptomatic, objectively confirmed VTE within 90 days. Patients whose physicians were alerted were more than twice as likely to receive VTE prophylaxis as control subjects (46.0% versus 20.6%; P<0.0001). The symptomatic VTE rate was lower in the intervention group (2.7% versus 3.4%; hazard ratio, 0.79; 95% CI, 0.50 to 1.25), but the difference did not achieve statistical significance. The rate of major bleeding at 30 days in the alert group was similar to that in the control group (2.1% versus 2.3%; P=0.68).
Conclusions: A strategy of direct notification of the physician by a staff member increases prophylaxis use and leads to a reduction in the rate of symptomatic VTE in hospitalized patients. However, VTE prophylaxis continues to be underused even after physician notification, especially among Medical Service patients.
Trial registration: ClinicalTrials.gov NCT00409136.
Conflict of interest statement
Gregory Piazza, MD- none
Erin J. Rosenbaum, BA- none
William Pendergast, MD- sanofi-aventis (Research Grant > $10,000, Speaker’s Bureau > $10,000, Consultant/Advisory Board < $10,000); Pfizer (Speaker’s Bureau < $10,000); Novartis (Speaker’s Bureau < $10,000)
Joseph O. Jacobson, MD- none
Robert C. Pendleton, MD- none
Gordon D. McLaren, MD- sanofi-aventis (Research Grant > $10,000); Bristol-Myers Squibb (Research Grant > $10,000)
C. Gregory Elliott, MD- none
Scott M. Stevens, MD- none
William F. Patton, MD- St. Joseph Mercy Health System (Honoraria < $10,000) Ousama Dabbagh, MD- Bristol-Myers Squibb (Research Grant > $10,000); Pfizer (Research Grant > $10,000); Missouri Society of Respiratory Therapists (Honoraria < $10,000)
Marilyn D. Paterno, MBI- none
Elaine Catapane, MEd, MT- none
Zhongzhen Li, MD- none
Samuel Z. Goldhaber, MD- sanofi-aventis (Research Grant > $10,000, Consultant/Advisory Board < $10,000); Eisai (Research Grant > $10,000, Consultant/Advisory Board < $10,000); Boehringer Ingelheim (Research Grant > $10,000, Consultant Advisory Board < $10,000); Bristol-Myers Squibb (Consultant Advisory Board < $10,000)
Figures

Comment in
-
Letter by Spyropoulos regarding article, "Physician alerts to prevent symptomatic venous thromboembolism in hospitalized patients".Circulation. 2009 Dec 15;120(24):e288. doi: 10.1161/CIRCULATIONAHA.109.884981. Circulation. 2009. PMID: 20008737 No abstract available.
References
-
- Kucher N, Koo S, Quiroz R, Cooper JM, Paterno MD, Soukonnikov B, Goldhaber SZ. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352:969–977. - PubMed
-
- Kucher N, Castellanos LR, Quiroz R, Koo S, Fanikos J, Goldhaber SZ. Time trends in warfarin-associated hemorrhage. Am J Cardiol. 2004;94:403–406. - PubMed
-
- Kearon C, Ginsberg JS, Hirsh J. The role of venous ultrasonography in the diagnosis of suspected deep venous thrombosis and pulmonary embolism. Ann Intern Med. 1998;129:1044–1049. - PubMed
-
- Stein PD, Fowler SE, Goodman LR, Gottschalk A, Hales CA, Hull RD, Leeper KV, Jr, Popovich J, Jr, Quinn DA, Sos TA, Sostman HD, Tapson VF, Wakefield TW, Weg JG, Woodard PK. Multidetector computed tomography for acute pulmonary embolism. N Engl J Med. 2006;354:2317–2327. - PubMed
-
- Bates DW, Gawande AA. Improving safety with information technology. N Engl J Med. 2003;348:2526–2534. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
