

Impact of a multifaceted intervention on cholesterol management in primary care practices: guideline adherence for heart health randomized trial
- PMID: 19364997
- PMCID: PMC2937279
- DOI: 10.1001/archinternmed.2009.44
Impact of a multifaceted intervention on cholesterol management in primary care practices: guideline adherence for heart health randomized trial
Abstract
Background: Physician adherence to National Cholesterol Education Program clinical practice guidelines has been poor.
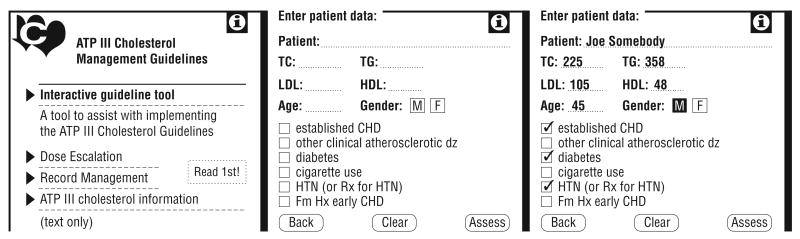
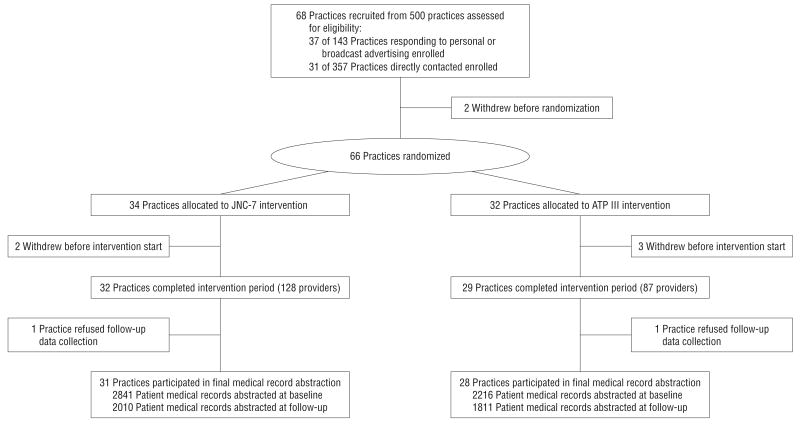
Methods: We recruited 68 primary care family and internal medicine practices; 66 were randomly allocated to a study arm; 5 practices withdrew, resulting in 29 receiving the Third Adult Treatment Panel (ATP III) intervention and 32 receiving an alternative intervention focused on the Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). The ATP III providers received a personal digital assistant providing the Framingham risk scores and ATP III-recommended treatment. All practices received copies of each clinical practice guideline, an introductory lecture, 1 performance feedback report, and 4 visits for intervention-specific academic detailing. Data were abstracted at 61 practices from random samples of medical records of patients treated from June 1, 2001, through May 31, 2003 (baseline), and from May 1, 2004, through April 30, 2006 (follow-up). The proportion screened with subsequent appropriate decision making (primary outcome) was calculated. Generalized estimating equations were used to compare results by arm, accounting for clustering of patients within practices.
Results: We examined 5057 baseline and 3821 follow-up medical records. The screening rate for lipid levels increased from 43.6% to 49.0% (ATP III practices) and from 40.1% to 50.8% (control practices) (net difference, -5.3% [P = .22]). Appropriate management of lipid levels decreased slightly (73.4% to 72.3%) in ATP III practices and more markedly (79.7% to 68.9%) in control practices. The net change in appropriate management favored the intervention (+9.7%; 95% confidence interval [CI], 2.8%-16.6% [P < .01]). Appropriate drug prescription within 4 months decreased in both arms (38.8% to 24.8% in ATP III practices and 45.3% to 24.1% in control practices; net change, +7.2% [P = .37]) Overtreatment declined from 6.6% to 3.9% in ATP III and rose from 4.2% to 6.4% in control practices (net change, -4.9% [P = .01]).
Conclusions: A multifactor intervention including personal digital assistant-based decision support may improve primary care physician adherence to the ATP III guidelines. Trial Registration clinicaltrials.gov Identifier: NCT00224848.
Figures
References
-
- LaRosa JC, He J, Vupputuri S. Effect of statins on risk of coronary disease: a meta-analysis of randomized controlled trials. JAMA. 1999;282(24):2340–2346. - PubMed
-
- Rosamond W, Flegal K, Friday G, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics—2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115(5):e69–e171. - PubMed
-
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III) JAMA. 2001;285(19):2486–2497. - PubMed
-
- Nieto FJ, Alonso J, Chambless LE, et al. Population awareness and control of hypertension and hypercholesterolemia: the Atherosclerosis Risk in Communities Study. Arch Intern Med. 1995;155(7):677–684. - PubMed
-
- Hoerger TJ, Bala MV, Bray JW, Wilcosky TC, LaRosa J. Treatment patterns and distribution of low-density lipoprotein cholesterol levels in treatment-eligible United States adults. Am J Cardiol. 1998;82(1):61–65. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
