

A comparison of pharmacologic and spontaneous baroreflex methods in aging and hypertension
- PMID: 19365284
- PMCID: PMC2745725
- DOI: 10.1097/HJH.0b013e32832a6e1b
A comparison of pharmacologic and spontaneous baroreflex methods in aging and hypertension
Abstract
Background: Phenylephrine bolus injection is an established technique to measure baroreflex sensitivity (BRS). This study quantified the relationship between the phenylephrine method and noninvasive measures of BRS and examined the effects of aging and hypertension on BRS. We also examined whether heart rate variability (HRV) provides as much information as does BRS.
Methods: BRS was determined by phenylephrine bolus (BRSphe), amyl nitrite inhalation (BRSamyl), Valsalva maneuver (BRSVals) and by time (BRS(+)) and spectral domain analysis (BRS(LFalpha), 004-015 Hz) of spontaneous blood pressure and R-R interval changes over the 5-min time period.
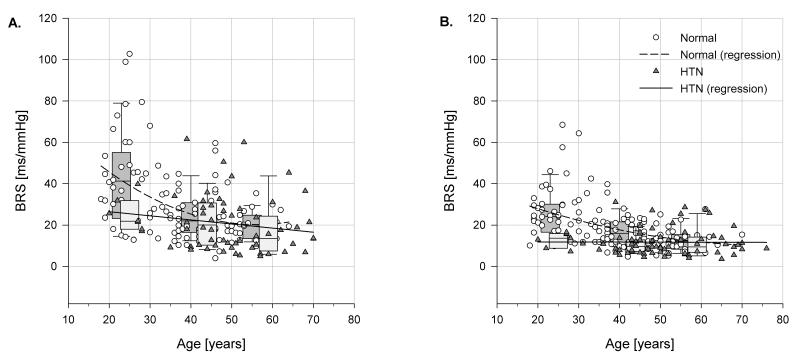
Results: The phenylephrine method significantly correlated with other methods (BRS(LFalpha) R = 0.54, BRS(+) R = 0.55, BRSVals R = 0.43 and BRSamyl R = 0.39; P < or = 0.001). Each method underestimated the BRSphe by the factors 0.62, 0.64, 0.59 and 0.33, respectively; P value less than 0.001. Only BRS(LFalpha) was significantly different between normotensive and hypertensive patients in young [24.3 +/- 1.4 (n = 40) vs. 12.2 +/- 2.3 (n = 7)] and middle-aged [16.5 +/- 1.1 (n = 71) vs. 10.8 +/- 1.1 (n = 31) groups, respectively]. HRV in the high frequency band (0.15-0.40 Hz) was significantly lower in young hypertensive patients than in normal controls (26 +/- 6.0 vs. 50 +/- 2.4, P < 0.05).
Conclusion: Although all methods correlated with the phenylephrine technique, none of them could be used interchangeably with that technique. BRS(LFalpha) detected the baroreflex loss of hypertension most clearly, and BRSamyl did not differ among groups.
Figures

References
-
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology Heart rate variability: standards of measurement, physiological interpretation, and clinical use. Circulation. 1996;93:1043–1065. - PubMed
-
- La Rovere MT, Bersano C, Gnemmi M, Specchia G, Schwartz PJ. Exercise-induced increase in baroreflex sensitivity predicts improved prognosis after myocardial infarction. Circulation. 2002;106:945–949. - PubMed
-
- La Rovere MT, Bigger JTJ, Jr, Marcus FI, Mortara A, Schwartz PJ. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. Lancet. 1998;351:478–484. - PubMed
-
- Smyth HS, Sleight P, Pickering GW. Reflex regulation of arterial pressure during sleep in man: a quantitative method of assessing baroreflex sensitivity. Circ Res. 1969;24:109–21. - PubMed
-
- Pagani M, Somers V, Furlan R, Dell’orto S, Conway J, Basselli G, et al. Changes in autonomic regulation induced by physical training in mild hypertension. Hypertension. 1988;12:600–610. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
