

Gene flow, subspecies composition, and dengue virus-2 susceptibility among Aedes aegypti collections in Senegal
- PMID: 19365540
- PMCID: PMC2663788
- DOI: 10.1371/journal.pntd.0000408
Gene flow, subspecies composition, and dengue virus-2 susceptibility among Aedes aegypti collections in Senegal
Abstract
Background: Aedes aegypti, the "yellow fever mosquito", is the primary vector to humans of the four serotypes of dengue viruses (DENV1-4) and yellow fever virus (YFV) and is a known vector of Chikungunya virus. There are two recognized subspecies of Ae. aegypti sensu latu (s.l.): the presumed ancestral form, Ae. aegypti formosus (Aaf), a primarily sylvan mosquito in sub-Saharan Africa, and Ae. aegypti aegypti (Aaa), found globally in tropical and subtropical regions typically in association with humans. The designation of Ae. aegypti s.l. subspecies arose from observations made in East Africa in the late 1950s that the frequency of pale "forms" of Ae. aegypti was higher in populations in and around human dwellings than in those of the nearby bush. But few studies have been made of Ae. aegypti s.l. in West Africa. To address this deficiency we have been studying the population genetics, subspecies composition and vector competence for DENV-2 of Ae. aegypti s.l. in Senegal.
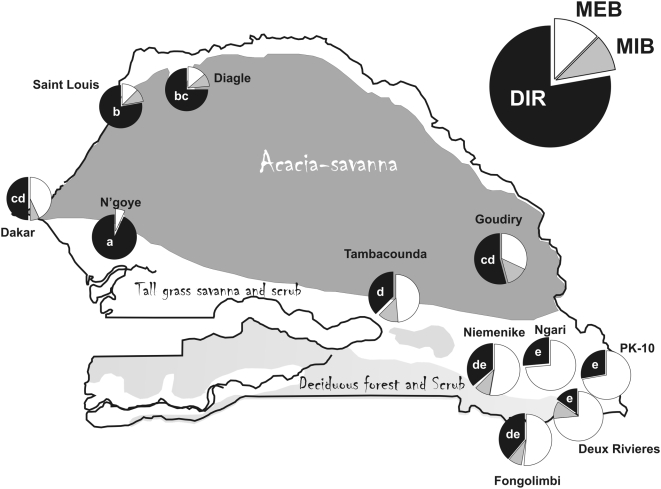
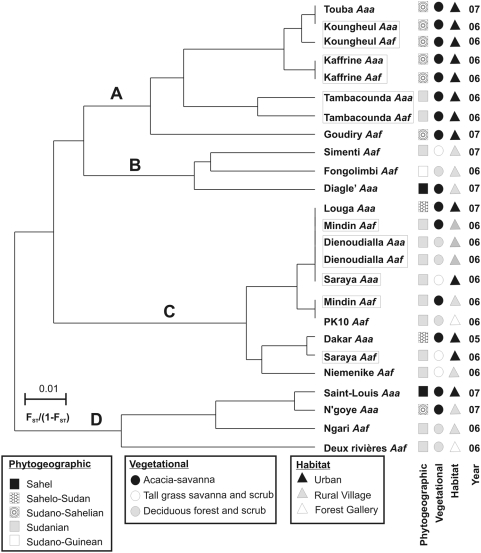
Methods and findings: A population genetic analysis of gene flow was conducted among 1,040 Aedes aegypti s.l. from 19 collections distributed across the five phytogeographic regions of Senegal. Adults lacking pale scales on their first abdominal tergite were classified as Aedes aegypti formosus (Aaf) following the original description of the subspecies and the remainder were classified as Aedes aegypti aegypti (Aaa). There was a clear northwest-southeast cline in the abundance of Aaa and Aaf. Collections from the northern Sahelian region contained only Aaa while southern Forest gallery collections contained only Aaf. The two subspecies occurred in sympatry in four collections north of the Gambia in the central Savannah region and Aaa was a minor component of two collections from the Forest gallery area. Mosquitoes from 11 collections were orally challenged with DENV-2 virus. In agreement with the early literature, Aaf had significantly lower vector competence than Aaa. Among pure Aaa collections, the disseminated infection rate (DIR) was 73.9% with a midgut infection barrier (MIB) rate of 6.8%, and a midgut escape barrier (MEB) rate of 19.3%, while among pure Aaf collections, DIR = 34.2%, MIB rate = 7.4%, and MEB rate = 58.4%. Allele and genotype frequencies were analyzed at 11 nuclear single nucleotide polymorphism (SNP) loci using allele specific PCR and melting curve analysis. In agreement with a published isozyme gene flow study in Senegal, only a small and statistically insignificant percentage of the variance in allele frequencies was associated with subspecies.
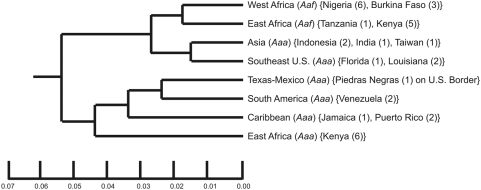
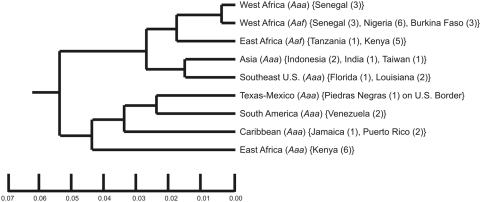
Conclusions: These results add to our understanding of the global phylogeny of Aedes aegypti s.l., suggesting that West African Aaa and Aaf are monophyletic and that Aaa evolved in West Africa from an Aaf ancestor.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




Similar articles
-
Vector competence in West African Aedes aegypti Is Flavivirus species and genotype dependent.PLoS Negl Trop Dis. 2014 Oct 2;8(10):e3153. doi: 10.1371/journal.pntd.0003153. eCollection 2014 Oct. PLoS Negl Trop Dis. 2014. PMID: 25275366 Free PMC article.
-
Morphology and taxonomic status of Aedes aegypti populations across Senegal.PLoS One. 2020 Nov 18;15(11):e0242576. doi: 10.1371/journal.pone.0242576. eCollection 2020. PLoS One. 2020. PMID: 33206725 Free PMC article.
-
Morphological and genetic variability within Aedes aegypti in Niakhar, Senegal.Infect Genet Evol. 2010 May;10(4):473-80. doi: 10.1016/j.meegid.2010.03.001. Epub 2010 Mar 16. Infect Genet Evol. 2010. PMID: 20223297
-
The distinctive bionomics of Aedes aegypti populations in Africa.Curr Opin Insect Sci. 2022 Dec;54:100986. doi: 10.1016/j.cois.2022.100986. Epub 2022 Oct 13. Curr Opin Insect Sci. 2022. PMID: 36243315 Review.
-
Aedes vittatus (Bigot) mosquito: An emerging threat to public health.J Vector Borne Dis. 2017 Oct-Dec;54(4):295-300. doi: 10.4103/0972-9062.225833. J Vector Borne Dis. 2017. PMID: 29460858 Review.
Cited by
-
Insecticide susceptibility of Aedes aegypti populations from Senegal and Cape Verde Archipelago.Parasit Vectors. 2012 Oct 22;5:238. doi: 10.1186/1756-3305-5-238. Parasit Vectors. 2012. PMID: 23088621 Free PMC article.
-
Quantitative analysis of replication and tropisms of Dengue virus type 2 in Aedes albopictus.Am J Trop Med Hyg. 2010 Sep;83(3):700-7. doi: 10.4269/ajtmh.2010.10-0193. Am J Trop Med Hyg. 2010. PMID: 20810842 Free PMC article.
-
Vector competence in West African Aedes aegypti Is Flavivirus species and genotype dependent.PLoS Negl Trop Dis. 2014 Oct 2;8(10):e3153. doi: 10.1371/journal.pntd.0003153. eCollection 2014 Oct. PLoS Negl Trop Dis. 2014. PMID: 25275366 Free PMC article.
-
Dengue Vectors and their Spatial Distribution.Trop Med Health. 2011 Dec;39(4 Suppl):17-27. doi: 10.2149/tmh.2011-S04. Epub 2011 Aug 25. Trop Med Health. 2011. PMID: 22500133 Free PMC article.
-
Arbovirus Epidemiology: The Mystery of Unnoticed Epidemics in Ghana, West Africa.Microorganisms. 2022 Sep 27;10(10):1914. doi: 10.3390/microorganisms10101914. Microorganisms. 2022. PMID: 36296190 Free PMC article. Review.
References
-
- Halstead SB, Suaya JA, Shepard DS. The burden of dengue infection. Lancet. 2007;369:1410–1411. - PubMed
-
- Tomori O. Yellow fever: The recurring plague. Crit Rev Clin Lab Sci. 2004;41:391–427. - PubMed
-
- Robertson SE, Hull BP, Tomori O, Bele O, LeDuc JW, et al. Yellow fever - A decade of reemergence. Jama-Journal of the American Medical Association. 1996;276:1157–1162. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
