

Outpatient weight loss surgery: initiating a gastric bypass and gastric banding ambulatory weight loss surgery center
- PMID: 19366541
- PMCID: PMC3015916
Outpatient weight loss surgery: initiating a gastric bypass and gastric banding ambulatory weight loss surgery center
Abstract
Background: Ambulatory surgery or outpatient surgery is becoming increasingly common. In 2002, 63% of all operations performed in the United States were ambulatory procedures. Bariatric procedures performed in the United States have increased from 16,200 in 1992 to approximately 205,000 in 2007. In 2002, our center began offering laparoscopic Roux-en-Y gastric bypass (LRYGB) procedures on an outpatient basis for select candidates at an ambulatory surgery center (ASC). We subsequently added laparoscopic adjustable gastric band procedures (LAGB) in 2005.
Methods: Between 2002 and 2008, 248 LRYGB and LAGB patients were carefully selected for ASC surgery by the bariatric surgeon and medical director. Extensive preoperative education was mandatory for all surgical candidates.
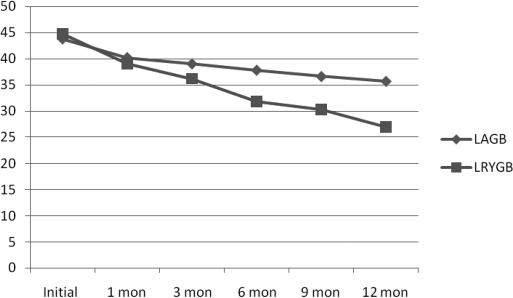
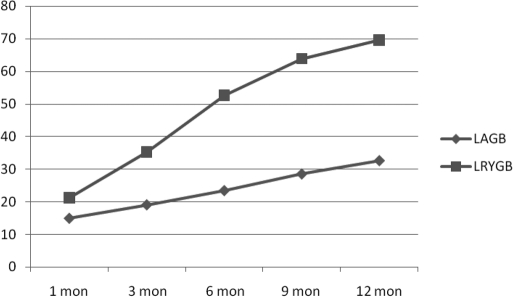
Results: Since 2002, we have performed 248 bariatric cases at the ASC, including 38 LRYGB and 210 LAGB procedures. In this overall experience, 5 patients (2%) required readmission within 30 days of surgery, and 98.6% of LAGB patients were discharged the same day; 62% were discharged after a 4-hour to 6-hour stay in the ASC. All LRYGB patients remained in the ASC overnight and were discharge within 24 hours of their procedure. Weight loss results have been excellent.
Conclusion: LAGB surgery can be safely performed in an ASC setting in most patients. LRYGB can be performed safely in the ASC setting with careful scrutiny and cautious selection of patient candidates.
Figures
References
-
- Dix K. Bariatric surgery: is this service right for you? Today's Surgicenter: Business Solutions for the ASC. October 5, 2007. Available at: http://www.surgicenteronline.com/articles/bariatric surgery.html Accessed October 20, 2007
-
- Adams TD, Gress RE, Smith SC, et al. Long-term mortality after gastric bypass surgery. N Engl J Med. 2007;357(8):753–761 - PubMed
-
- Sjostrom L, Narbro K, Sjostrom CD, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357(8):741–752 - PubMed
-
- Bray GA. The missing link - lose weight, live longer. N Engl J Med. 2007;357(8):818–820 - PubMed
-
- Russo CA, Owens P, Steiner C, Josephsen J. Ambulatory surgery in U.S. hospitals, in 2003. Fact book no. 9. U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality; Available at: http://www.ahrq.gov/data/hcup/factbk9/factbk9a.htm Accessed October 20, 2007
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous