

Review
Appendiceal inversion: a diagnostic and therapeutic dilemma
Affiliations
- PMID: 19366551
- PMCID: PMC3015910
Item in Clipboard
Review
Appendiceal inversion: a diagnostic and therapeutic dilemma
JSLS.
2009 Jan-Mar.
Abstract
Appendiceal inversion is an uncommon entity that presents a diagnostic dilemma for the gastroenterologist or surgeon. We present 2 cases that illustrate scenarios that may be encountered during colonoscopy. A discussion of the literature on this subject is also presented. An improved awareness of this condition will assist the endoscopist in the identification of this finding and direct the appropriate expectant management.
Figures
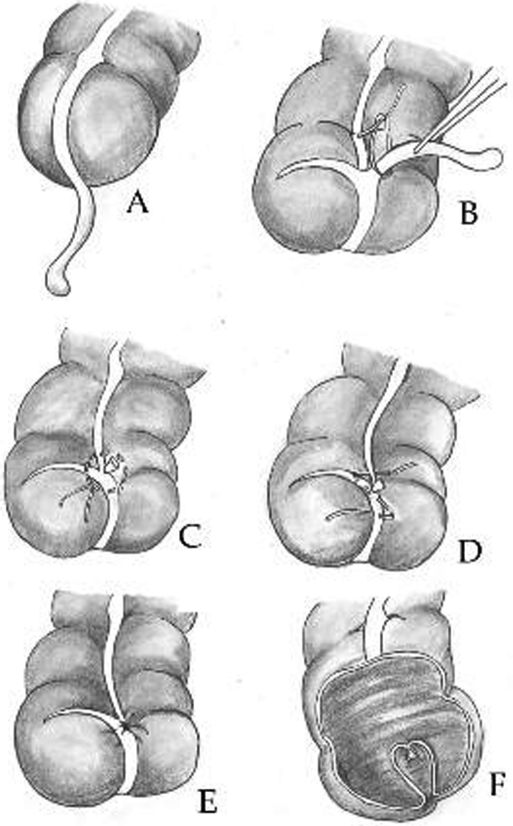
Appendiceal inversion procedure. After the base of the appendix (A) is ligated (B) and cut, a seromuscular purse-string suture (C) or a “Z” stitch (D) is placed around the stump. The appendiceal stump is then buried and the suture is tied (E). When the stump is inverted in the lumen of the intestine, it appears as a polypoid lesion entirely covered by mucosa (F).

Endoscopic photograph depicting the polypoid appearance of the appendiceal orifice.
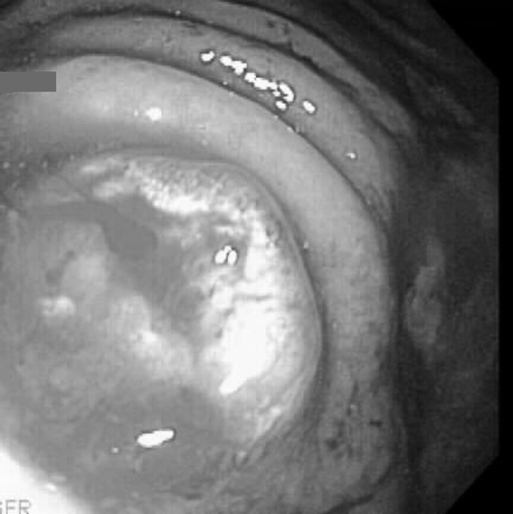
Endoscopic photograph depicting the remaining “stalk” after attempted snare polypectomy.
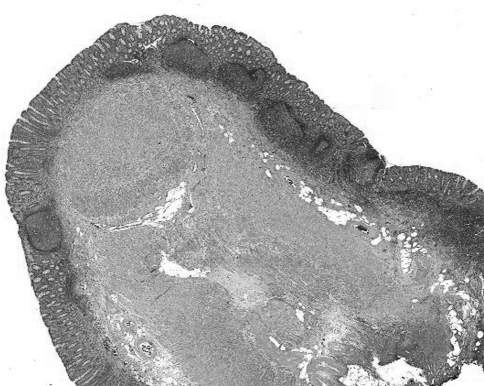
Inverted appendiceal stump lined by colonic type mucosa with prominent lymphoid follicles. The underlying muscularis propria appears hypertrophic. (hematoxylin-eosin, original magnification ×20).
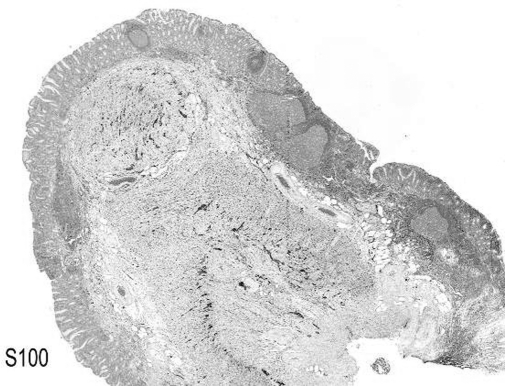
Prominent neurogenic component highlighted by anti S-100. (Immunohistochemistry using anti-S-100, original magnification ×20).
References
-
- Jevon GP, Daya D, Oizilbash AH. Intussusception of the appendix. A report of four cases and review of the literature. Arch Pathol Lab Med. 1992;116(9):960–964 - PubMed
-
- Voeller GR, Fabian TC. Inversion-ligation appendectomy for incidental appendectomy. Am J Surg. 1991;161(4):483–484 - PubMed
-
- Van Fleet RH, Shabot JM, Halpert RD. Adenocarcinoma of the appendiceal stump. South Med J. 1990;83:1351–1353 - PubMed
-
- Shami VM, Yerian LM, Waxman I. Adenoma and early stage adenocarcinoma of the appendix: diagnosis by colonoscopy. Gastrointest Endosc. 2004;59:731–733 - PubMed
-
- Hardin RD. Colonoscopic diagnosis of an appendiceal polyp with carcinoma in situ. J Clin Gastroenterol. 1986;8:189–191 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources