

Ranirestat for the management of diabetic sensorimotor polyneuropathy
- PMID: 19366965
- PMCID: PMC2699746
- DOI: 10.2337/dc08-2110
Ranirestat for the management of diabetic sensorimotor polyneuropathy
Abstract
Objective: Aldose reductase inhibitors (ARIs) are potential disease modifiers for diabetes complications. We aimed to determine whether ranirestat, an ARI, could slow or reverse the course of diabetic sensorimotor polyneuropathy (DSP).
Research design and methods: A total of 549 patients with DSP were randomly assigned to treatment with placebo or 10, 20, or 40 mg/day ranirestat for 52 weeks in this multicenter, double-blind study. Efficacy was evaluated by nerve conduction studies, the modified Toronto Clinical Neuropathy Score (mTCNS), and quantitative sensory tests (QSTs).
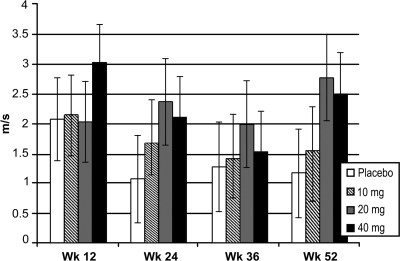
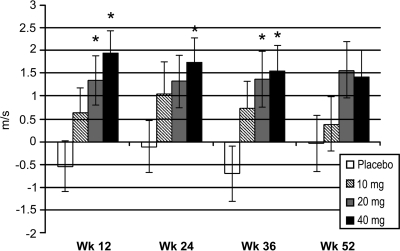
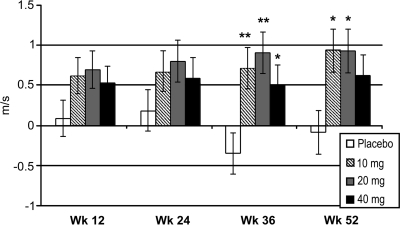
Results: At week 52, the summed sensory (bilateral sural plus proximal median sensory) nerve conduction velocity (NCV) did not show significant changes from baseline (2.0 m/s for placebo compared with 3.2-3.8 m/s for ranirestat). Significant improvement in the summed motor (peroneal, tibial, and median) NCV was observed with 20 and 40 mg/day ranirestat treatment at week 12 (P <or= 0.05) and at weeks 24 and 36 and in peroneal motor NCV at weeks 36 and 52 (P <or= 0.05) for the 20 mg/day ranirestat group. The mTCNS and QST results did not differ among the groups during the study. Ranirestat was well tolerated with no pertinent differences in drug-related adverse events or in effects on clinical laboratory parameters, vital signs, or electrocardiograms among the four groups.
Conclusions: Treatment with ranirestat appears to have an effect on motor nerve function in mild to moderate DSP, but the results of this study failed to show a statistically significant difference in sensory nerve function relative to placebo.
Trial registration: ClinicalTrials.gov NCT00101426.
Figures
References
-
- Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein JM, Pach D, Wilson DM, O'Brien PC, Melton LJ, III. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: the Rochester Diabetic Neuropathy Study. Neurology 1993; 43: 817– 824 - PubMed
-
- De Wytt C, Jackson RV, Hockings GI, Joyner JM, Strakosch CR. Polyneuropathy in Australian outpatients with type II diabetes mellitus. J Diabetes Complications 1999; 13: 74– 78 - PubMed
-
- Oates PJ. Polyol pathway and diabetic peripheral neuropathy. Int Rev Neurobiol 2002; 50: 325– 392 - PubMed
-
- Greene DA, Arezzo JC, Brown MB. Zenarestat Study Group. Effect of aldose reductase inhibition on nerve conduction and morphometry in diabetic neuropathy. Neurology 1999; 53: 580– 591 - PubMed
-
- Pfeifer MA, Schumer MP. Clinical trials of diabetic neuropathy: past, present, and future. Diabetes 1995; 44: 1355– 1361 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
