

Secular trends in diabetes-related preventable hospitalizations in the United States, 1998-2006
- PMID: 19366966
- PMCID: PMC2699731
- DOI: 10.2337/dc08-2211
Secular trends in diabetes-related preventable hospitalizations in the United States, 1998-2006
Abstract
Objective: To examine secular trends in diabetes-related preventable hospitalizations among adults with diabetes in the U.S. from 1998 to 2006.
Research design and methods: We used nationally representative data from the National Inpatient Sample to identify diabetes-related preventable hospitalizations. Based on the Agency for Healthcare Research and Quality's Prevention Quality Indicators, we considered that hospitalizations associated with the following four conditions were preventable: uncontrolled diabetes, short-term complications, long-term complications, and lower-extremity amputations. Estimates of the number of adults with diabetes were obtained from the National Health Interview Survey. Rates of hospitalizations among adults with diabetes were derived and tested for trends.
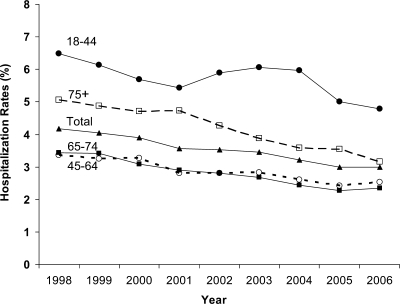
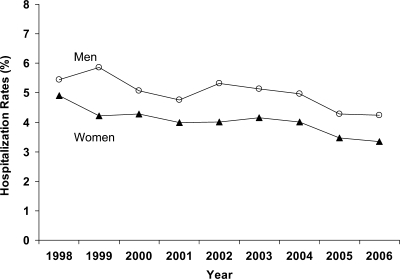
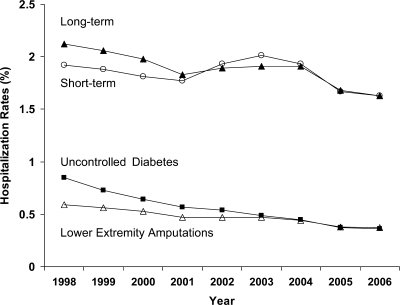
Results: Age-adjusted rates for overall diabetes-related preventable hospitalizations per 100 adults with diabetes declined 27%, from 5.2 to 3.8 during 1998-2006 (P(trend) < 0.01). This rate decreased significantly for all but not for short-term complication (58% for uncontrolled diabetes, 37% for lower-extremity amputations, 23% for long-term complications [all P < 0.01], and 15% for the short-term complication [P = 0.18]). Stratified by age-group and condition, the decline was significant for all age-condition groups (all P < 0.05) except short-term complications (P = 0.33) and long-term complications (P = 0.08) for the age-group 18-44 years. The decrease was significant for all sex-condition combination subgroups (all P < 0.01).
Conclusions: We found a decrease in diabetes-related preventable hospitalizations in the U.S. from 1998 to 2006. This trend could reflect improvements in quality of primary care for individuals with diabetes.
Figures
Similar articles
-
Schizophrenia and potentially preventable hospitalizations in the United States: a retrospective cross-sectional study.BMC Psychiatry. 2013 Jan 25;13:37. doi: 10.1186/1471-244X-13-37. BMC Psychiatry. 2013. PMID: 23351438 Free PMC article.
-
Factors Contributing to Increases in Diabetes-Related Preventable Hospitalization Costs Among U.S. Adults During 2001-2014.Diabetes Care. 2019 Jan;42(1):77-84. doi: 10.2337/dc18-1078. Epub 2018 Nov 19. Diabetes Care. 2019. PMID: 30455326 Free PMC article.
-
Trends in quality of primary care in the United States, 2007-2016.Sci Rep. 2022 Feb 7;12(1):1982. doi: 10.1038/s41598-022-06077-y. Sci Rep. 2022. PMID: 35132143 Free PMC article.
-
Geographic Variation in Potentially Preventable Hospitalizations for Acute and Chronic Conditions, 2005–2011.2014 Sep. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb–. Statistical Brief #178. 2014 Sep. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb–. Statistical Brief #178. PMID: 25411684 Free Books & Documents. Review.
-
Potentially Preventable Pediatric Hospital Inpatient Stays for Asthma and Diabetes, 2003–2012.2015 Jun. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb–. Statistical Brief #192. 2015 Jun. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb–. Statistical Brief #192. PMID: 26312368 Free Books & Documents. Review.
Cited by
-
Racial and Ethnic Disparities in Preventable Hospitalizations for Chronic Disease: Prevalence and Risk Factors.J Racial Ethn Health Disparities. 2017 Dec;4(6):1100-1106. doi: 10.1007/s40615-016-0315-z. Epub 2016 Dec 6. J Racial Ethn Health Disparities. 2017. PMID: 27924622 Review.
-
Revisiting risks associated with mortality following initial transtibial or transfemoral amputation.J Rehabil Res Dev. 2012;49(10):1479-92. doi: 10.1682/jrrd.2012.02.0030. J Rehabil Res Dev. 2012. PMID: 23516052 Free PMC article.
-
Trends in hospitalization of patients with diabetes mellitus in Ghana from 2012 to 2017 with predictions to 2032.Int Health. 2022 Nov 1;14(6):588-596. doi: 10.1093/inthealth/ihab076. Int Health. 2022. PMID: 34849982 Free PMC article.
-
The impact of ambulatory care spending, continuity and processes of care on ambulatory care sensitive hospitalizations.Eur J Health Econ. 2022 Nov;23(8):1329-1340. doi: 10.1007/s10198-022-01428-y. Epub 2022 Jan 29. Eur J Health Econ. 2022. PMID: 35091856 Free PMC article.
-
Quantifying Geographic Variation in Health Care Outcomes in the United States before and after Risk-Adjustment.PLoS One. 2016 Dec 14;11(12):e0166762. doi: 10.1371/journal.pone.0166762. eCollection 2016. PLoS One. 2016. PMID: 27973617 Free PMC article.
References
-
- American Diabetes Association. Economic costs of diabetes in the U.S. in 2007. Diabetes Care 2008; 31: 596– 615 - PubMed
-
- Bindman AB, Grumbach K, Osmond D, Komaromy M, Vranizan K, Lurie N, Billings J, Stewart A: Preventable hospitalizations and access to health care. JAMA 1995; 274: 305– 311 - PubMed
-
- Billings J, Zeitel L, Lukomnik J, Carey TS, Blank AE, Newman L: Impact of socioeconomic status on hospital use in New York City. Health Aff 1993; 12: 162– 173 - PubMed
-
- Agency for Healthcare Research and Quality. AHRQ Quality Indicators—Guide to Prevention Quality Indicators: Hospital Admission for Ambulatory Care Sensitive Conditions. Version 3.1. Rockville, MD, Agency for Healthcare Research and Quality, 2001. ( AHRQ Publ. No. 02-R0203)
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
