

The impact of healthcare costs in the last year of life and in all life years gained on the cost-effectiveness of cancer screening
- PMID: 19367281
- PMCID: PMC2676546
- DOI: 10.1038/sj.bjc.6605018
The impact of healthcare costs in the last year of life and in all life years gained on the cost-effectiveness of cancer screening
Abstract
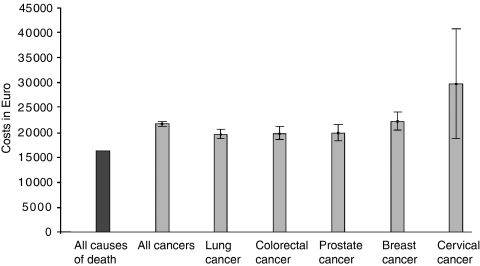
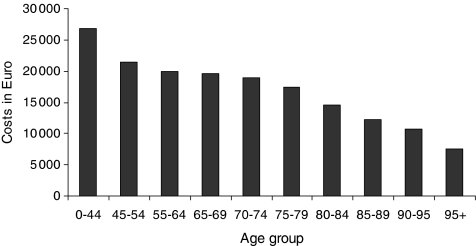
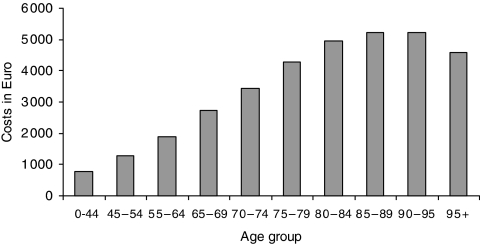
It is under debate whether healthcare costs related to death and in life years gained (LysG) due to life saving interventions should be included in economic evaluations. We estimated the impact of including these costs on cost-effectiveness of cancer screening. We obtained health insurance, home care, nursing homes, and mortality data for 2.1 million inhabitants in the Netherlands in 1998-1999. Costs related to death were approximated by the healthcare costs in the last year of life (LastYL), by cause and age of death. Costs in LYsG were estimated by calculating the healthcare costs in any life year. We calculated the change in cost-effectiveness ratios (CERs) if unrelated healthcare costs in the LastYL or in LYsG would be included. Costs in the LastYL were on average 33% higher for persons dying from cancer than from any cause. Including costs in LysG increased the CER by 4040 euro in women, and by 4100 euro in men. Of these, 660 euro in women, and 890 euro in men, were costs in the LastYL. Including unrelated healthcare costs in the LastYL or in LYsG will change the comparative cost-effectiveness of healthcare programmes. The CERs of cancer screening programmes will clearly increase, with approximately 4000 euro. However, because of the favourable CER's, including unrelated healthcare costs will in general have limited policy implications.
Figures
References
-
- Eakin EG, Youlden DR, Baade PD, Lawler SP, Reeves MM, Heyworth JS, Fritschi L (2007) Health behaviors of cancer survivors: data from an Australian population-based survey. Cancer Causes Control 18: 881–894 - PubMed
-
- Gandjour A, Lauterbach KW (2005) Does prevention save costs? Considering deferral of the expensive last year of life. J Health Econ 24: 715–724 - PubMed
-
- Garber AM, Phelps CE (1997) Economic foundations of cost-effectiveness analysis. J Health Econ 16: 1–31 - PubMed
-
- Garber AM, Weinstein MC, Torrance GW, Kamlet MS (1996) Theoretical foundations of cost-effectiveness analysis. In Cost-Effectiveness in Health and Medicine, Gold MR, Russel L, Weinstein M (eds) pp 45–47. University Press: Oxford
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
