

Treatment options in patients with rheumatoid arthritis failing initial TNF inhibitor therapy: a critical review
- PMID: 19368701
- PMCID: PMC2669237
- DOI: 10.1186/ar2666
Treatment options in patients with rheumatoid arthritis failing initial TNF inhibitor therapy: a critical review
Abstract
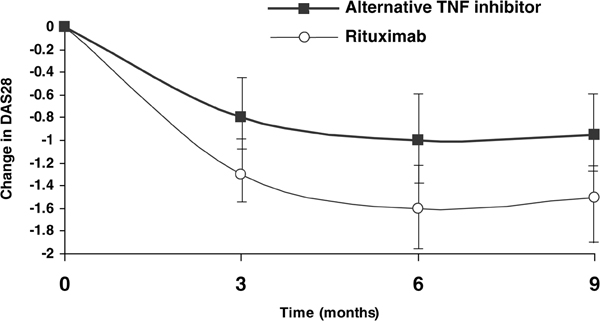
Conventional disease-modifying antirheumatic drugs such as methotrexate are the mainstay of treatment for rheumatoid arthritis. More recently, biologic agents such as etanercept, infliximab and adalimumab, which act by inhibiting tumour necrosis factor (TNF), have become available. TNF inhibitors have proved to be very effective in patients not responding to conventional disease-modifying antirheumatic drugs. However, about 20% to 40% of patients treated with a TNF inhibitor fail to achieve a 20% improvement in American College of Rheumatology criteria, and more lose response over time (secondary failure or acquired therapeutic resistance) or experience adverse events following treatment with a TNF inhibitor. In this group of patients, therapeutic options were limited until recently and an established treatment approach was to switch from one TNF inhibitor to another. In recent years, therapeutic options in these patients have increased with the introduction of biologic agents with novel mechanisms of action, such as rituximab and abatacept. This review outlines the current evidence in support of the available treatment strategies in patients with an inadequate response or intolerance to an initial TNF inhibitor.
Figures
References
-
- Pincus T, Kavanaugh A, Sokka T. Benefit/risk of therapies for rheumatoid arthritis: underestimation of the 'side effects' or risks of RA leads to underestimation of the benefit/risk of therapies. Clin Exp Rheumatol. 2004;22(suppl 35):S2–S11. - PubMed
-
- Emery P, Genovese MC, Kavanaugh AF, Cohen SB, Perez JL, Sasso EH. Adalimumab plus methotrexate results in less frequent and less severe radiographic progression than methotrexate alone at all levels of clinical response in early rheumatoid arthritis [abstract] Ann Rheum Dis. 2006;65(suppl II):88.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
